



Revealing the Stark Reality of School Transmission: Clear Airborne Threat as JN.1 Asserts Global Dominance Amidst Increasing Hospitalizations
"JN.1 is the Most Immune Evading Variant to Date." China is taking steps to protect children in schools. We'll look at the measures they are putting in place.

As the newly dominant JN.1 variant sweeps across the U.S. and around the world, a recent study offers stark insights into the limitations of our current testing strategies, the alarming prevalence of airborne transmission and the silent spread of COVID-19 in children.
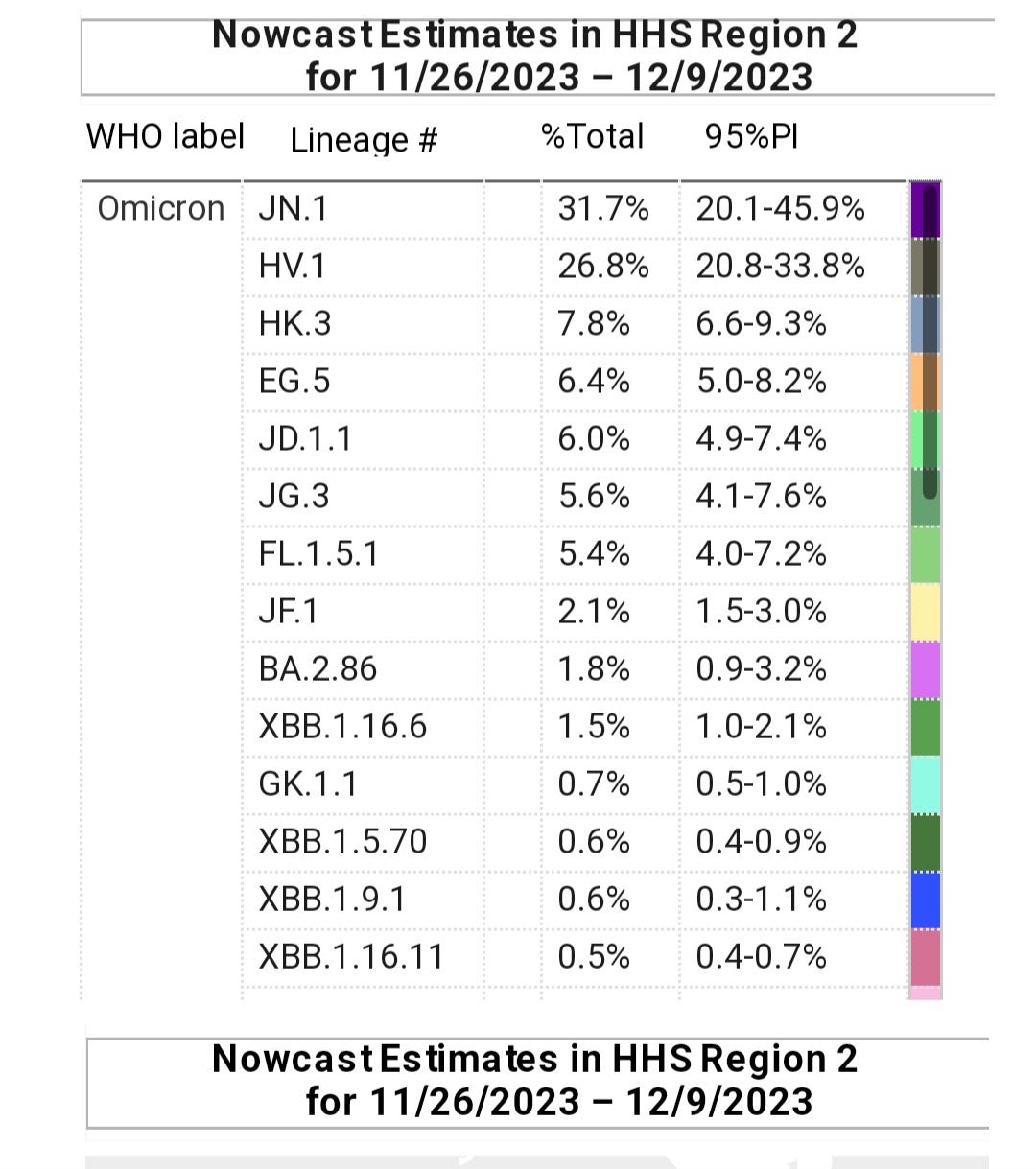
The CDC updated it’s variant proportions on December 8, 2023 and it shows, as we predicted, the JN.1 variant becoming dominant in the Northeast U.S. and closing in quickly in the rest of the country. JN.1 is likely above 60% of cases in many countries around the world. We will explore China’s strategies in managing in-school transmission and look at the surge of hospitalizations in Italy and Singapore. As JN.1 continues to expand its reach working its way up through the age groups to older adults, hospitals should anticipate and brace for a surge in hospitalizations set to escalate exponentially until between early and mid-January.
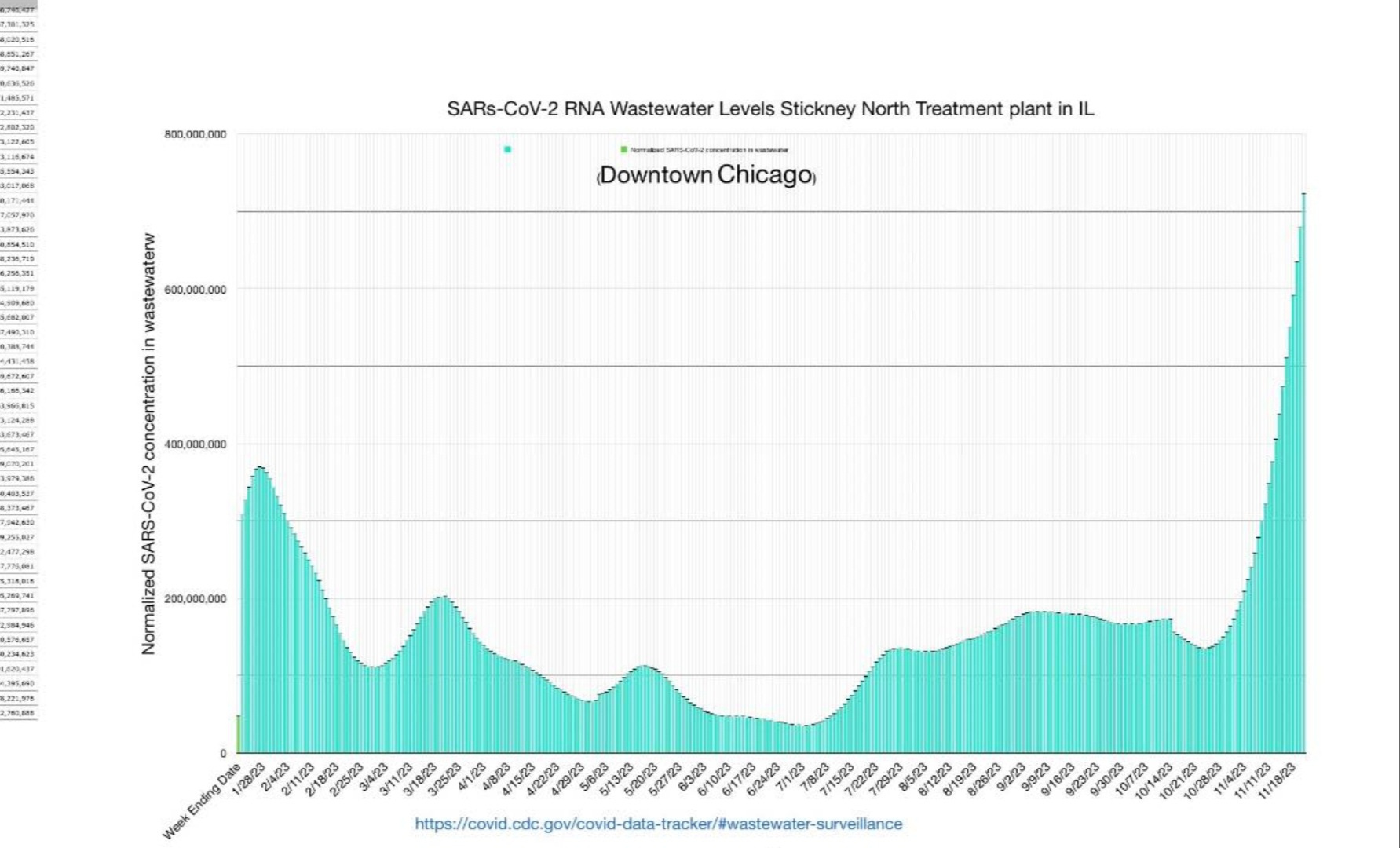
⚠️ With several more weeks of unchecked growth ahead and wastewater levels at record highs in various regions, brace yourself for what could be the most infectious wave of the entire pandemic, both in the U.S. and worldwide, leading to weakened immune systems, secondary infections, and persistent COVID infections. ⬅️
We can hope that this doesn’t happen but many indications are pointing in this direction so being prepared is essential.
We will also highlight the latest study showing that the JN.1 variant evades the neutralizing antibodies induced by the XBB.1.5 targeted vaccine. While this revelation might not startle seasoned TACT readers, it serves as a solid confirmation of our expectations. Join us as we unravel the details of this crucial report.
By becoming a paid subscriber, you're not only gaining access to exclusive content but also actively supporting the future of this important work. Contribute to our mission by becoming a valued paid subscriber today.
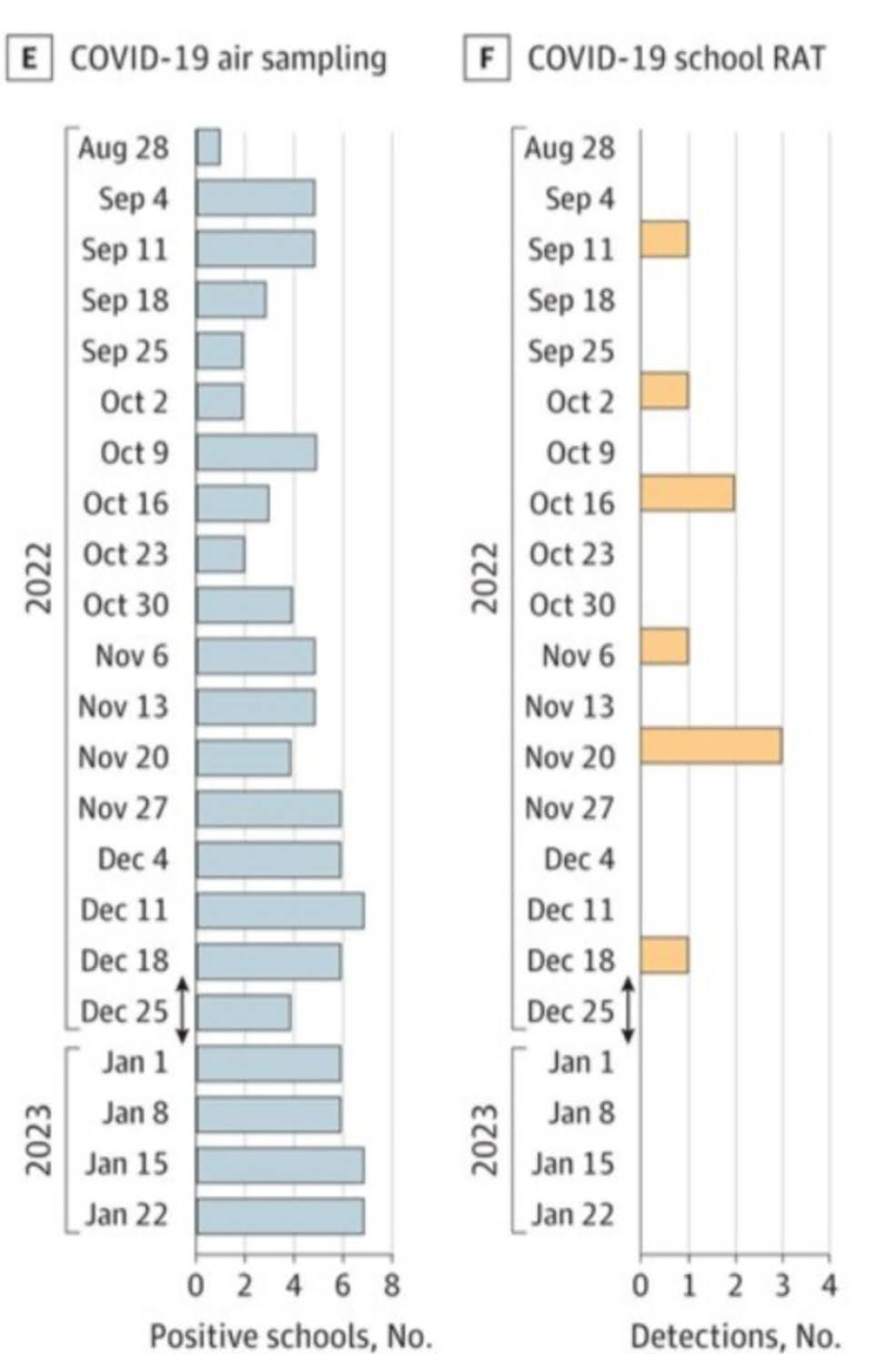
A study published December 5, 2023, focused on air sampling and three other testing methods to show differences between testing methods and the prevalence in the air across multiple schools of a school district in Wisconsin. This study reveals a number of alarming truths about the virus's silent spread and the limitations of current testing methods.
Rapid Antigen Tests Miss the Mark:
The study, conducted in Wisconsin schools, found that rapid antigen tests (RAT), the mainstay of at-home and school testing programs, are woefully inadequate. Their inability to detect COVID until 4 to 5 days after exposure or symptom onset means they miss a significant number of infections while children are having the most symptoms, as we can see below.
The RAT negative results within the first few days, when children and young adults are most severely impacted, creates a false sense of security likely contributing to the continued spread of the virus.
The study's findings reinforce the need for comprehensive testing strategies that go beyond rapid tests to capture a more accurate picture of COVID prevalence in schools.
The rapid tests aren't recorded at your doctors office unless visiting or you make a special point to share the results. Many people won't connect the dots to having COVID and chalk it up to aging or something else. Without any proof of injury, it makes it much harder to qualify for disability insurance, should that need arise. If you find yourself in that situation, you will understand why the “free tests” are not free.
Airborne Threat is Very High in Schools:
Utilizing air sampling technology, the study paints a disturbing picture of COVID's presence in the air of schools. The virus lingers in classrooms, hallways, and cafeterias, far exceeding the levels of influenza.
This widespread airborne transmission poses a significant health risk to students and staff, highlighting the need for better ventilation and air filtration systems.
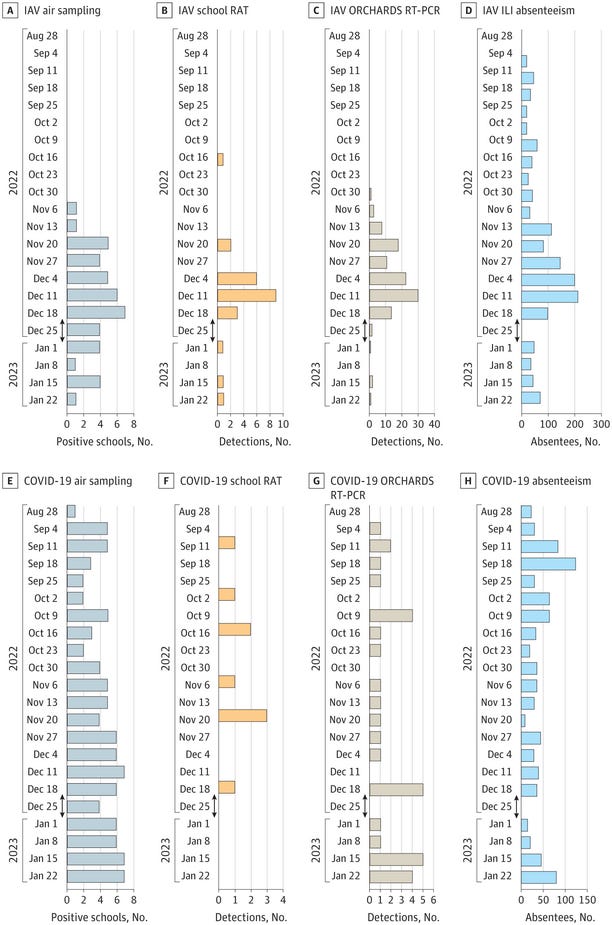
Preventable Airborne Viruses Result in Excessive Absenteeism
COVID, RSV and flu are all large contributors to absenteeism every year. COVID is significantly increasing the level of absenteeism. TACT reported on Nov. 5, 2023, a “doubling of the chronic absenteeism rate (in the U.S.) since before the pandemic, reaching 29.7% in 2022 from 16.2% in 2019. This crisis has affected over 14 million students, up from 8 million before the pandemic. High chronic absenteeism levels not only impact absent students but also affect everyone in the classroom, including teachers.”
“This issue places a significant burden on schools, making it difficult for teachers to meet the needs of all students, juggling efforts to catch up absen tees while keeping other students engaged. In the 2021-22 school year, they showed that 43% percent of schools had extreme levels of chronic absence. “Elementary schools were especially affected with extreme chronic absence jumping from 7% to 38% of all elementary schools.” Maybe now we can understand that COVID is having a much larger impact on children than any other virus.
As shown in the graphic below, absenteeism attributed to the flu is showing up “before” influenza is found in the air. If a COVID test comes back negative from the school nurse, doctor or at home, then often parents will consider the reason for the absence to be the flu. This can be attributed to the rapid antigen tests producing a negative result. COVID is shown to be present in the air at the time of those absences.
This is particularly important now as JN.1 becomes dominant in the Northeast U.S. and around the world. JN.1 has strategically altered its approach, skillfully evading the acquired immunity induced by the XBB variants, which has been a shield for many over the past year. The consequences of this tactical shift are elevating the risks associated with COVID-related complications.
Before delving into the global impact of JN.1, let's hear from Dr. Sean Mullen, a research director, who amplifies the key points mentioned earlier and introduces new perspectives. His insights, shared on Twitter/X, encapsulate the essence of the Wisconsin school study, providing a crucial backdrop to our review.
⚠️ Unseen Danger in Our Schools:
"A recent Wisconsin study exposes a disturbing reality – our kids are exposed to flu and COVID in schools more than what’s been realized!"
Here's what they found and why it's a wake-up call:
1️⃣ "Mixed Methods, Alarming Results: The study used home samples, rapid tests, absentee records, and air sampling. The findings? A steady presence of COVID alongside flu peaks, especially in winter months."
2️⃣ "The Invisible Threat: Air sampling revealed a constant exposure to COVID in schools. Detected flu in schools for 43 weeks, and COVID for 101 weeks! This isn't just about a virus; it's about our children's long-term health and cognitive well-being."
3️⃣ "Absences Tell a Tale: Over 2,300 combined absences due to flu-like symptoms and COVID (880 Covid+). It's not just numbers; these are days of education and normal childhood lost."
4️⃣ "Ignored Alarms: The persistence of COVID in school environments is not just alarming but a call to action. Where are the infrastructure improvements for better air quality in schools?"
"We can't stay silent. This study sheds light on a critical issue that's being overlooked. Our kids deserve safe schools. It's time for tangible action, not just words. Improved air quality in schools isn't a luxury; it's a necessity."
School Transmission Continued
A study published November 2021, with the study period from July to Oct 2020, on COVID prevalence in children under 19 yrs old in Virginia, found "66% of seropositive children had no symptoms of COVID-19.” They concluded that children had a much higher burden of COVID infections, when compared to the adults in the same region at the same time.
“The role of children’s disease transmission must be considered in COVID-19 mitigation strategies"
Key Takeaways on School Transmission
1. Silent Spread: A surprising 66% of children with COVID-19 antibodies showed no symptoms, indicating widespread asymptomatic transmission. This likely contributed to underestimating the true infection rate among children.
2. Children are at Higher Risk: Compared to adults in the same region, children carried a significantly higher burden of COVID-19 infection. This contradicts earlier assumptions and highlights their vulnerability.
3. Children as Vectors: These studies challenge the prior beliefs of many people and suggest that children play a significant role in COVID-19 transmission. This necessitates revised mitigation strategies.
4. Widespread Airborne Transmission: Multiple studies, including the most recent one using air samplers, confirm the extensive airborne presence of COVID-19 and other respiratory viruses within schools. This poses a significant health risk for students and staff.
5. Impact Beyond Health: School outbreaks of influenza, RSV, COVID-19 and other respiratory pathogens lead to high absenteeism, disrupting learning, impacting work productivity, and increasing healthcare costs.
6. The Need for Action: Preventing airborne transmission of these viruses in schools holds immense potential to benefit individuals, families, and the entire community. This includes protecting children's health, ensuring educational continuity, boosting economic productivity, and reducing healthcare costs.
7. Urgent Call to Action: The widespread evidence of airborne transmission in schools demands immediate prioritization of preventative measures by government officials and school boards. Implementing effective strategies to shield students and staff from airborne pathogens must be a top priority. Help support the Clean Air for Kids campaign.

China is Taking Action to Prevent Transmission in Schools
Meanwhile in China, they are working to protect children and stop transmission in schools. That sounds like a very logical thing to do. Why isn't that happening in Europe or the U.S.?
The South China Morning Post is reporting on Dec. 7, 2023, that "China’s education ministry has urged schools to step up daily health checks and reporting as the country grapples with a wave of respiratory illness among children.”
In a directive issued on Monday, it also said schools should conduct risk assessments with local health departments to help fight the problem. They said that if a third of students in one class were sick, they would suspend classes and that schools should report it to the local disease control departments.
In the directive, the education ministry told schools to make preparations for online classes for sick children and guide them in home learning.
It also said schools should “guide families in disease control”
“Too many kids are sick. Some parents send their kids to school even when they’re sick, so that the kids won’t miss classes,” one concerned parent told the Post."
This sounds familiar.
They reported a 35-year-old designer in Wuhan, said “he was really worried when his three-year-old daughter needed hospital treatment after coming down with a mycoplasma infection.”
“The CAT scan revealed that half of her lung was white. It’s the first time since she was born that she’s been sick so badly”
Another parent said, “her son in primary school had contracted pneumonia in mid-November as a result of the flu and a mycoplasma infection, and has yet to recover.”
Surge of JN.1 in Singapore Sparks Hospitalization and ICU Concerns
Singapore's Ministry of Health (MOH) reported a significant jump in Covid-19 cases, hospitalizations, and ICU admissions in the week of November 26th to December 2nd.
Cases: 32,035 infections were estimated, a 45% increase from the 22,094 cases reported the previous week.
Hospitalizations: Average daily admissions rose to 225, a 65% increase from the previous week's 136.
ICU admissions: Average daily entries increased to 4 cases, a 300% increase compared to the 1 case reported the week before.
JN.1 variant: The JN.1 variant makes up over 60% of cases in Singapore.
Although MOH reassured that the numbers remain lower than the pandemic peak, they acknowledged the strain it placed on the already busy healthcare system.
The updated Covid-19 - XBB.1.5 targeted, monovalent, Pfizer and Moderna vaccines have been available at MOH’s joint testing and vaccination centers, since November 2023, and they continue to be free.
Vaccine Effectiveness
Unfortunately, these vaccines fall short in preventing infections or Long COVID and are unlikely to provide significant protection against severe disease. Regrettably, we lack data demonstrating their efficacy in boosting the memory T-cell response or ensuring that spike-specific T-cells effectively target the JN.1 variant. This is concerning because there's a possibility that these vaccines might obstruct an efficient immune response to the JN.1 variant by inducing antibodies that don’t prevent infection, and T-cells that don’t target it which could then become overactivated, potentially hindering the body's defenses.
As demonstrated in the Wisconsin study highlighted above, airborne transmission is rampant in crowded indoor spaces. Consequently, nearly everyone has been exposed multiple times to the XBB variants succeeding XBB.1.5. This renders the use of a vaccine targeting XBB.1.5 virtually pointless, or even counterproductive, potentially undermining the body's established defenses. The current challenge arises from the fact that the JN.1 variant evolved independently from the XBB variants, nullifying the immunity previously acquired and the protection that shielded most individuals over the past year.
The latest study to show that the vaccine induced antibodies won’t prevent infection was published Dec 8, 2023, and it says, “JN.1 shows robust resistance to monovalent XBB.1.5 vaccine sera compared to BA.2.86."
"Taken together, these results suggest that JN.1 is one of the most immune-evading variants to date. "
"Our results suggest that S:L455S contributes to increased immune evasion, which partly explains the increased Re of JN.1"
Overview of TACT’s Reporting on BA.2.86 and JN.1 (BA.2.86.1.1)
TACT first reported on BA.2.86 August 18th. On September 30th stated, “BA.2.86 prevalence is still quite low but it is here and it is spreading at a faster pace. All of this data points to it having a very real chance of becoming a serious problem going into November and December.”
From the October 15, 2023, TACT forecast, “We should prepare for a surge similar to the 2021/2022 Omicron surge that could extend into the first or second week of January. The most likely scenario is that the Pirola family surge will be milder than 2021/2022 but substantially higher than the 2022/2023 surge”
TACT reported in the November 5th update, the “Cumulative data suggests that the JN.1 sub-variant of BA.2.86 has the potential to become a global dominant variant.”
On Nov. 27th, TACT reported that COVID, influenza, RSV, Norovirus and other pathogens are spreading at an exponential pace, which means every week the prevalence and risk is growing significantly. This will continue until winter break.
On Nov. 28th, TACT reported, the BA.2.86 sub-variants will very likely become dominant, displacing the XBB variants descendent’s within the next week or two.”
On Nov. 30th, TACT reported that the mysterious pneumonia cases surging around the world matched the timing and subsequent rise of the BA.2.86 sub-variants, primarily, the JN.1 variant. TACT’’s hypothesis is that the likely culprit of the pneumonia is due to the multitude of new mutations in the BA.2.86 variants. The studies indicate it has an enhanced ability to attack respiratory epithelial cells, coupled with the highest immune evasion and suppression to date, resulting in a surge in both primary and secondary lung infections.
Due to the rapid transmission through schools, as shown above, children are the first impacted by new variants, like JN.1. This is likely why we are seeing the pneumonia outbreaks in children first. The study also shows why school officials aren’t detecting COVID when using the RAT tests.
The CDC updated the variant proportions on Dec. 8th, showing the JN.1variant becoming dominant in the Northeast U.S.
TACT’s Overview
Rapid Dominance: JN.1 is on the fast track to becoming the dominant variant worldwide, potentially achieving this status within the next week.
Exponential Growth: With an alarming doubling rate of approximately, every 8 to 9 days, JN.1 is likely surpassing the 50% mark in many locations, historically leading to an acceleration of prevalence.
Viral Load Dynamics: More infections translate to higher viral loads in individual spaces, creating a cycle where increased viral loads contribute to more infections within those spaces.
Risk Amplification: Elevated viral loads pose a heightened risk, as high-dose exposures make it tougher for the body to mount an effective defense.
Age Group Progression: JN.1 is progressing through age groups, with imminent implications for older adult communities and care facilities. Brace for a surge in hospitalizations and unfortunately, a potential rise in fatalities in the coming weeks.
Hospital Preparedness: Hospitals should be on high alert, preparing for a likely scenario of increased patient influx and heightened medical demands.
Coinfection Concerns: Amidst the JN.1 surge, communities also grapple with the prevalence of flu, RSV, and norovirus, raising the specter of co-infections. The compounded severity of co-infections adds to the risks of unmitigated transmission.
Prevention is the Best Medicine
"Strategies to Avoid COVID and Other Respiratory Viruses"
COVID Simplified:
Antibody Limitations: Antibodies do not fully block infection.
Reduced Symptoms: Many people experience fewer symptoms because the immune system is less effective, marked by increased evasion and suppression.
Secondary Infection Risk: The likelihood of secondary infections, such as M. pneumonia, is higher. The first symptoms may be that of the secondary infection, indicating a current or recent infection with the JN.1 variant.
Susceptibility Increase: There's an elevated risk of persistent infections and organ dysfunction due to a compromised immune system.
Challenge of Higher Viral Loads: Higher viral load exposures make it harder for the body to fight, escalating overall risks.
Italy

Chicago
Feel free to pose a question, share insights, or provide any helpful information you may have.
We have decent ventilation in my district, as at the start of the pandemic our union negotiated ventilation standards (8 exchanges per hour). They checked them often, offered hepa filters for older buildings or those that wanted them. I don't see them checking the ventilation any more, but it's still in our contract, so they continue. I have 2 district provided hepa filters in my classroom, I keep the windows open and my 2 ceiling fans going all year. My aide and I both wear masks, but none of my students do. Besides me, there are only 2 adults who wear masks, and both do this to humor me as neither wear them elsewhere. I'll take what I can get. Despite these precautions, my students are sick constantly, some over and over again. Recently, I'm also noticing a cognitive decline in a few students that is very concerning. It's not just a change in their academic abilities, but a loss of ability to make connections, to critically think, to figure out simple solutions to small problems. I've done Alzheimers care as a former nurse, and that's what it reminds me of. When I share this with my admin and other staff in the building, they point to the lockdown 2 years ago. We're in a liberal school, in a liberal district, in a blue city, in a blue state and the disconnect and gaslighting is still unreal. I don't see a change happening anytime soon and believe we are headed for disaster.
Hi TACT...So there is something that really struck me when I was looking at one of the tables you presented. Now, I haven't read the paper so maybe I am missing something. Take a look and compare Column E and Column G from the Wisconsin School Study. Column E suggests persistent levels of virus in the schools being measured and yet Column G tends to suggest that RT-PCR is less efficient at picking it up than the air sampling. For example, the peak in RT-PCR occurs on December 18th whereas school absenteeism has been going on for months prior to that peak. The trend looks like it might be starting to get better at the end of the study in January...perhaps the testing labs switched PCR amplification primers which resulted in better detection by that point. The virus may be mutating faster than appropriate primers can be developed to detect it.
Regarding the new XBB booster vaccine, you might find this study of interest if you haven't seen it.
https://www.biorxiv.org/content/10.1101/2023.11.28.569129v1