



The Cause of the Mysterious Pneumonia Surging in China, South Korea, France, Netherlands, Denmark and the U.S. is Revealed
We uncover what's behind the surge in respiratory illnesses. How concerning is it? Hint: It was necessary to provide an updated forecast.

In bustling megacities like Beijing, hospitals are grappling with an influx of children battling severe respiratory infections such as pneumonia. Despite the alarming situation, the Chinese government maintains there's no new pathogen at play. According to official statements, the surge in respiratory infections is attributed to typical winter coughs and colds, exacerbated by the relaxation of strict COVID-19 restrictions in December 2022. The World Health Organization (WHO), the CDC, the ECDC, and major media outlets echo these assurances, raising concerns that they have not learned from the past or just want to entertain a narrative that doesn’t cause alarm or any change in behavior that could disrupt the world economy.
We are taking a deeper dive, solving the mystery that governments and major media are largely ignoring by following the science and utilizing real world data. The evidence is growing and the probability is high that the underlying, mysterious, cause of the abnormal growth in respiratory infections leading to pneumonia, whooping cough and other issues is a virus. Bacterial pneumonia is often secondary to viral infections. Bacteria like that causing mycoplasma pneumonia are usually opportunistic, in that they take advantage of an immune system that has been weakened by a virus. So, for instance, influenza, RSV and the common cold can sometimes lead to bronchitis or pneumonia, infections of the upper and lower respiratory tract, respectively. We know that COVID can cause more damage to the immune system than the other viruses.
There are quite a few COVID variants causing illness, hospitalization and death, but there is one that has been increasing in prevalence at the same pace as the increasing cases of what are likely secondary respiratory infections. We will lay out the compelling evidence. The answer and scope of this will likely surprise you but you can be the judge. Answer the poll question at the end to let us know what you think.
If you haven't already increased your level of mitigation measures, now is the time to consider doing so. COVID, Influenza, RSV, Norovirus and other pathogens are rapidly expanding in prevalence with COVID having the highest rate of transmission. With real-world data aligning with scientific findings, the likelihood of this variant being the underlying issue is very high.
By becoming a paid subscriber, you're not only gaining access to exclusive content but also actively supporting the future of this important work. Contribute to our mission by becoming a valued paid subscriber today.
In case you haven’t already figured it out, we will review why the Pirola (BA.2.86) family of variants is the likely cause of the "mysterious" pneumonia in China, France, South Korea, the Netherlands, the U.S., and likely many other places. We will show that each of these countries is seeing pneumonia and other respiratory infections surge at the same pace as the BA.2.86 variants within each country.
We still need China's variant proportions to confirm, but this is likely happening worldwide based on the data presented here and in the TACT article from November 29, 2023.
The Pirola variant family, represented by BA.2.86, is rapidly expanding its presence, approaching an estimated 38% prevalence globally. BA.2.86 is antigenically distinct from XBB.1.5 and previous XBB variants, allowing it to escape XBB-induced neutralizing antibodies. There is a good reason to believe they will evade the immunity enjoyed for the past year or more to the XBB variants to which nearly everyone has been exposed at least once but likely many times to lower doses that didn't cause symptoms.
The Pirola variants are likely to cause more harm, particularly in the lungs.
BA.2.86 variants, with JN.1 (BA.2.86.1.1) leading the way, have an increased capacity to infect respiratory epithelial cells combined with extreme immune evasion & suppression. This combination of changes increases the likelihood of seeing increasing respiratory symptoms from both JN.1 & secondary infections. China, France, South Korea, the Netherlands and now the U.S., are all seeing surges of pneumonia primarily in children that surpass the earlier pandemic years.
Real World Data
Let’s look at some of the articles reporting on the situation in the various countries impacted, including France, China, South Korea, the Netherlands, Denmark and the U.S.
France:
"In France, an increase in lung infections caused by the bacterium Mycoplasma pneumoniae has been recorded in recent days.” The cases mainly concern minors under the age of 15, but it is working its way up through the age group's as shown in Netherlands data. "In this age group, last week there was a 36 percent increase in medical consultations for this type of infection. A similar trend has not been recorded in the country for about ten years." (1)
➡️ " Symptoms are similar to those of the flu or coronavirus, with fever, fatigue and cough."(1)
China:
"Thus far, Chinese officials say causal agents include known pathogens, such as mycoplasma, RSV, influenza and SARS-CoV-2 (the virus that causes Covid-19)." (2)
"Among other countries, China, South Korea and France are having serious epidemics, and the suspected main culprit appears to be mycoplasma pneumonia." (2)
South Korea:
"In South Korea, confirmed cases of the illness more than doubled from mid October to mid November. According to a summary released by the Korean Agency for Disease Control and Prevention, 226 (96%) of the 236 hospitalized patients with acute bacterial respiratory infections during the second week of November had mycoplasma pneumonia. Notably, 80% of new patients are children under age 5." (1)
Netherlands:
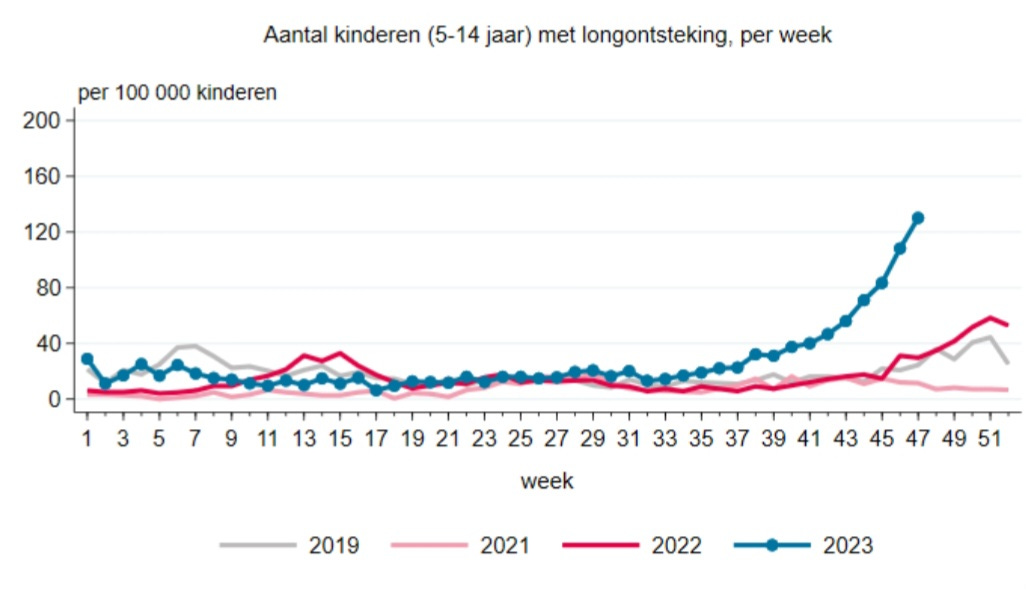
There are a striking number of children and young people with pneumonia. In week 47 (Nov 20-26), the number of children aged 5 to 14 with pneumonia increased to 130 per 100,000 children. Last year there were 58 per 100,000 children at its peak.
General Practitioners also see more pneumonia in the group of young people between the ages of 15 and 24 than in previous years. In week 47, this number further increased to 38 per 100,000.
History as shown us that in periods of exponential growth, COVID is expanding through schools and homes, working its way up through the age groups. The Netherlands data shows that this is expanding into the older age groups. The trend will likely continue for the next 4 to 6 weeks. In other words, this will likely make its way to older adults in the coming weeks. Sadly, that is when hospitalizations and deaths will rapidly increase.

(Note: The language is Dutch so to clarify, Pneumonia is represented in the graph above and Pertussis, also known as whooping cough, in the graph below)

The number of children who visited the General Practitioner (GP) for whooping cough is higher than the previous three years.
Since week 34, there has been an upward trend in the number of patients with whooping cough in the 0 to 14 age group.
“In weeks 45,46, and 47, or in other words, the first 3 weeks of November, the number of children with whooping cough is increasing sharply compared to the weeks before.
The Netherlands has a very small sample size of testing so it is impossible to draw conclusions solely based on the following information, but the viruses they found in the 55 samples that were taken are RSV: 8 times (14.5%), SARS-CoV-2: 7 times (13%), Rhinovirus: 5 times (9%), Influenza virus: 2 times (4%), Parainfluenzaviruses: 1 time (2%), Seasonal coronaviruses: 1 time (2%). Even among this small sample, the top two viruses are RSV and COVID.
They say that as far as SARS-CoV-2, “There has been a slow upward trend in the number of patients with SARS-CoV-2 (COVID-19) at the GP since week 34, but since week 40, the number of patients has been fairly stable.”(3)
Ohio, U.S.A:
An article, published Nov. 29, 2023 from Fox19, says that in Warren County Ohio, more children are getting sick with pneumonia across multiple school districts and that they have not been able to narrow down the source or the cause. The is eerily similar to the mysterious pneumonia in China and France? They said that started “roughly in August, but really picking up in mid-late October, and we’ve been noticing a lot of cases of kids being absent and the resulting diagnosis being Pneumonia.”(4) Take note of the August start to this outbreak. Weeks 33 and 34 are the last two weeks of August and as we will see below, it is also the precise time frame that cases of BA.2.86 started being recorded across Europe and in the U.S.
The three pathogens they have discovered “thus far in their research: Mycoplasma pneumonia, Streptococcus pneumonia, and Adenovirus." This sounds very similar to France, Netherlands, and China, but they left out any mention of COVID. This isn’t surprising considering doctors are less likely to test for it and reporters are less likely to include it, in many areas of the U.S.
They said the average age thus far is 8 years old in Ohio. We know from France the ages primarily impacted are under 15 years old. In the Netherlands, they are seeing cases primarily under 15 years old but increasing in 15 to 24 years as well. It is expanding up through the age groups.
Conclusions “A much higher burden of SARS-CoV-2 infection, as determined by seropositivity, was found in children than previously reported; this was also higher compared to adults in the same region at a similar time. Contrary to prior reports, we determined children shoulder a significant burden of COVID-19 infection. The role of children’s disease transmission must be considered in COVID-19 mitigation strategies” (5) (published:1/28/2021)
Denmark:
“Danish medical institute declares ‘cold pneumonia’ epidemic” “In a statement released on Wednesday, November 29, the medical entity announced that an increasing number of Danes had tested positive for the respiratory infection Mycosplasma pneumoniae. As a result, the situation could be categorised as an epidemic it confirmed”(6)
“Hanne-Dorthe Emborg, a senior researcher at SSI, explained that there were ‘significantly more cases than usual’.”(6)
The information that is lacking from these reports.
We need to know, how often are they testing for COVID?
What type of tests are they using?
Do they recognize that the rapid antigen tests normally won’t detect COVID until the 4th or 5th day from the start of symptoms?
Additionally, why haven't manufacturers made the tests a little more sensitive considering we have known about the delay in testing positive for a couple years?
If COVID is discovered, how soon after COVID started are the secondary infections taking place?
Review of the increasing prevalence of BA.2.86 variants and the increasing cases of pneumonia
Remember this, week 34 is the last week of August and it is a key piece of the puzzle because that is the start of both the increasing prevalence of BA.2.86 variants and the start of the increasing cases of pneumonia.
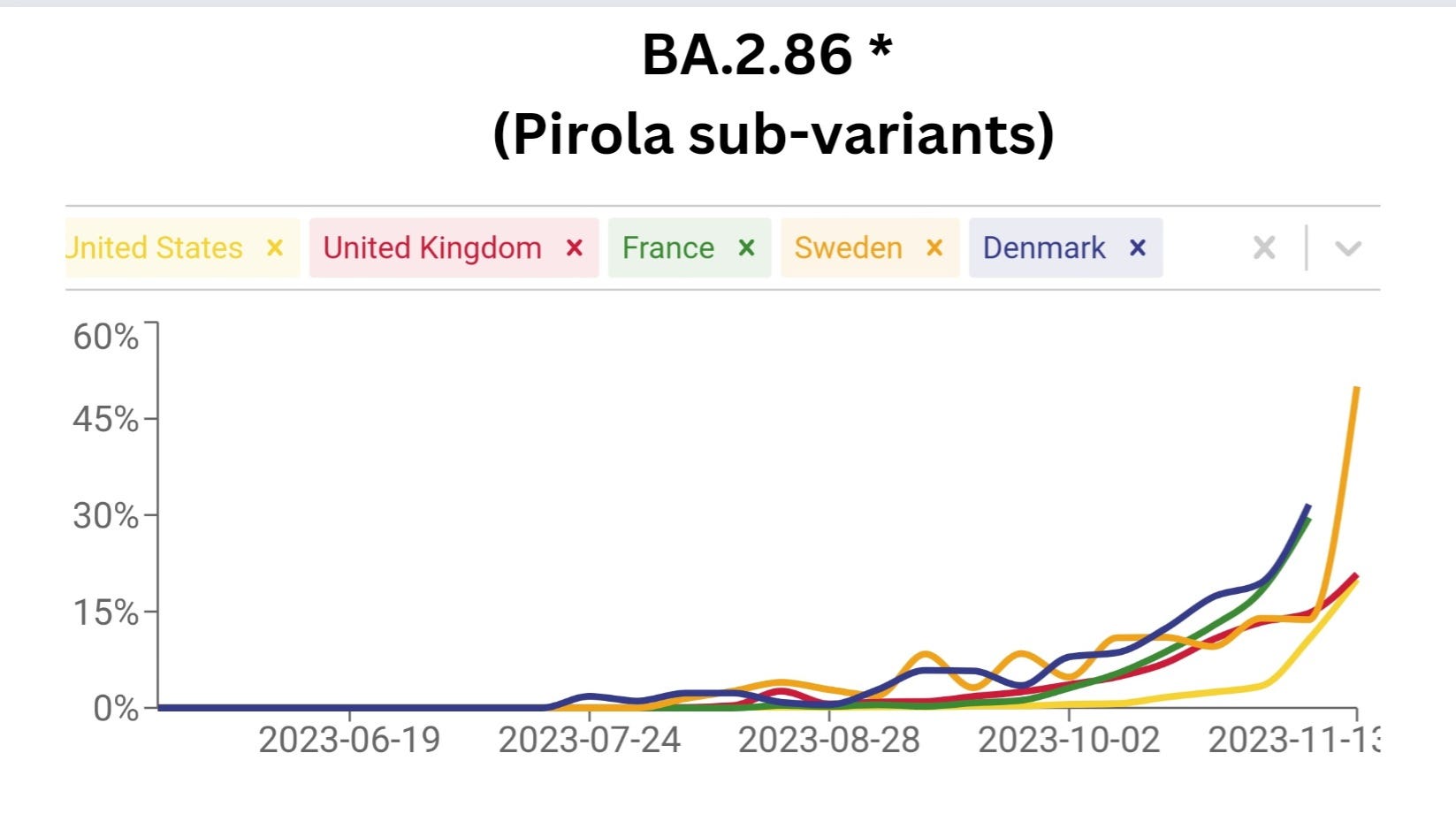
If we look at the prevalence of BA.2.86 variants increasing in France, the Netherlands, and the U.S., we see that the weeks of increasing prevalence align with the increase in pneumonia and pertussis (whooping cough).
Note: week 34 is where the pneumonia cases in the Netherlands separated from the norm, and has continued increasing from there. Week 34 is the last week of August, precisely when Wisconsin started seeing the increase in pneumonia and the same time BA.2.86 started increasing.

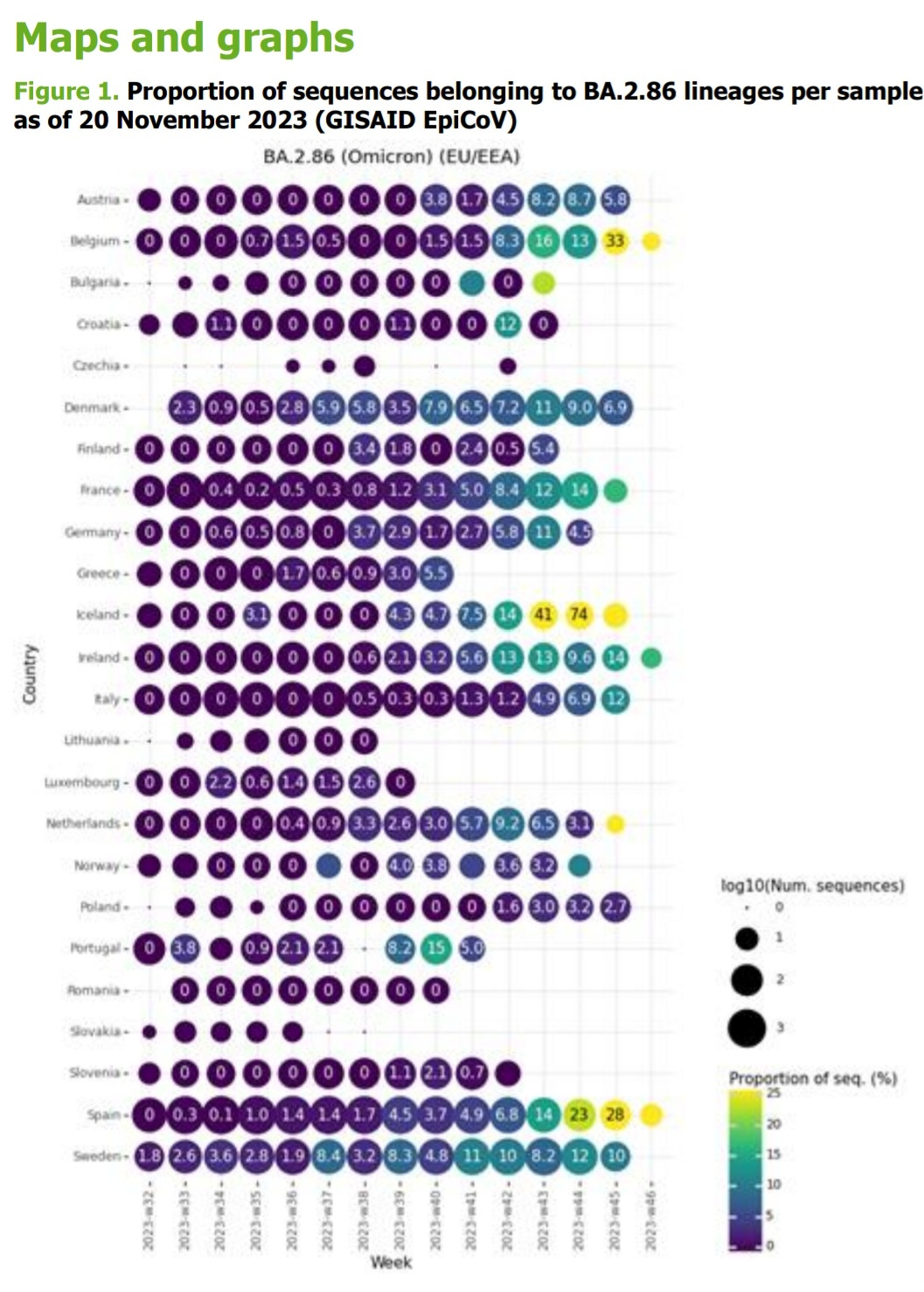
From the ECDC on BA.2.86'S prevalence per country.
First detected and growing exponentially from week 34 in France and week 36 in the Netherlands. This is with decreased sequencing and the delay in reporting the results.
The Science
This excerpt is extracted from yesterday's article dated November 29, 2023. You can access the complete article here.
(Note: The points discussed herein are derived from studies presented on November 29, 2023. It's important to note that the insightful and likely reliable studies are in the pre-peer review stage for full disclosure. Nevertheless, these findings are crucial for current discussion given the timeframes involved in the peer review process.)
BA.2.86 - The Pirola Family of Variants are Likely to Cause:
Increased infectivity in the lungs and respiratory tract.
If the virus can enter lung cells more efficiently, it could lead to a higher concentration of the virus in the lungs, potentially resulting in more severe respiratory symptoms.
Impact on Symptoms:
If the virus gains entry into cells faster and replicates swiftly, it could accelerate the appearance of symptoms from the time of exposure.
Early symptoms, beyond body aches, fever, chills, and headaches, may encompass an elevated probability of experiencing a runny nose, sneezing, mild cough, or breathing difficulties.
Subsequent symptoms, potentially heightened by these variants, involve the loss of smell or taste, more severe respiratory manifestations, brain fog, and prolonged neurological and cognitive issues.
The Fox19 article on the Ohio outbreak certainly eludes to the expected change in symptoms described in the November 29, 2023 article and this is important to know. “I think parents need to know that if their child is exhibiting symptoms, including shortness of breath, rapid breathing, significant coughing where they’re unable to catch their breath, that they need to reach out to their pediatrician or their provider to have the child evaluated,” said Dr. Koenig.
BA.2.86 Variants and the Potential Implications
(This section is excerpts from the article yesterday, November 29, 2023. You can access that full article here. If you read this already, you can skip to the next section.)
Genetic Differences:
The BA.2.86 variant has different genetic instructions compared to other versions of the virus, with 36 unique mutations, including 32 substitutions, 3 deletions, and 1 insertion.
Some of these changes make it better at avoiding the body's natural defenses. Mutations like I332V, K356T, V445H, N450D, N481K, A484K, and 483del on BA.2.86's Receptor Binding Domain (RBD) are likely to enhance immune evasion.
The number of genetic changes in the BA.2.86 variant, compared to BA.2 and XBB.1.5, is similar to the number of changes observed in the initial Omicron strains when compared to the original Wu-Hu-1 strain.
Immune Evasion Mechanism:
The virus has developed a more efficient way to hide from the body's immune system, making it harder for our defenses to recognize and fight it.
Specific changes in the virus help it hide better and also affect how it attaches to our cells. We will dive into this in more detail in another study below.
Antibody Resistance:
The virus can resist the effects of the antibodies our body produces to fight it and prevent it from infecting our cells.
Even the antibodies that worked against other versions of the virus, like the XBB variants, may not work as well or not at all against this new variant.
BA.2.86 is antigenically distinct from XBB.1.5 and can escape neutralizing antibodies induced by XBB variants.
Vaccine Implications:
The BA.2.86 sub-variants might be different enough that vaccines, which were designed for older versions, may not work as effectively against it.
Faster Entry and Persistent Infections:
The cell membrane route involves the virus directly fusing with the cell membrane to enter the host cell. This direct fusion might be a quicker process compared to the endosomal route, which involves the virus being taken up by the cell in a vesicle (endosome) before releasing its genetic material.
Increased risk of viral persistence. Combined with the greater immune evasion and suppression, faster entry means faster replication, more time to circulate, and infiltrate into viral reservoirs throughout the body and brain before T-cells can eliminate the infected cells.
TACT’s Overview:
It’s possible that the increasing cases of bacterial and viral respiratory infections leading to pneumonia and pertussis is the cumulative toll of weakened immune systems from many COVID infections, but consider this. China, with fewer COVID infections per person, compared to the Netherlands, Denmark, France, or the U.S., is experiencing a simultaneous increase in pneumonia cases, that is coinciding with the prevalence of the BA.2.86 variants in all the other countries.
When science aligns closely with real-world data, the likely culprit is the multitude of new mutations in the BA.2.86 variants, that the studies indicate has an enhanced ability to attack respiratory epithelial cells, coupled with the highest immune evasion and suppression to date. We end up with a surge in secondary lung infections. It's crucial to note that for every pneumonia case, there are likely many times greater number of infections by these variants. The evasion and suppression of the immune system may lead to fewer initial symptoms, with secondary infections becoming the primary indicators in many cases.
This situation poses a significant risk of persistent infections, potentially leading to Long COVID and disabling conditions for millions. For those that avoid Long COVID, there is an increased odds of musculoskeletal, neurological, vascular and cognitive dysfunction. People will have less time until conditions arise that diminish the quality of life and ultimately this shortens lifespans through multiple mechanisms. (See COVID Accelerated Aging, How many years of life are we losing from COVID infections?)
The severity of health conditions is influenced by the viral load someone is exposed to, and with insufficient upgrades to ventilation and air filtration, the risk of infection remains high. Considering the likelihood of less noticeable initial symptoms with these variants, more people could be contagious without detectable signs.
There are things we can do and now is the time to do them.
“Strategies to Avoid COVID and Other Respiratory Viruses. Prevention is the Best Medicine”
Updated Forecast:
We should prepare for a surge similar to the 2021/2022 Omicron surge in prevalence and transmission that could extend into the first or second week of January with hospitalizations continuing to build for another one to two weeks.
Contrary to expectations, the Pirola variant surge may not be milder than 2021/2022. It is likely to be substantially higher than the 2022/2023 surge as is already indicated by CDC wastewater data. Starting in mid-January, we should see exponential decay continuing into February.
Hospitals should brace for a significant influx of patients in the coming weeks.
Cumulative data suggests that the JN.1 sub-variant of BA.2.86 has the potential to become a global dominant variant. The current trends indicate its ascent coincides with the exponential spread of COVID, flu, RSV, and other pathogens posing a high-risk scenario for millions.
Anticipate a significant increase in secondary infections, such as pertussis, mycoplasma pneumonia, streptococcus pneumonia, influenza, RSV and adenovirus, impacting the lungs more harshly, through immune suppression than any prior variant.
Given our limited understanding of this variant's impact on children's developing brains, lungs and immune system, taking immediate steps to reduce the transmission of airborne viruses in schools and safeguarding healthcare settings is of critical importance.
Purely anecdotal: my daughter tested positive for covid on Sept 20. She's 35 and has mild asthma, but is otherwise healthy and fit. On Sept 28 she tested negative. She felt better. At the beginning of Nov, she started coughing again, and she was diagnosed with "post covid pneumonia" . She has been on several antibiotics and they don't seem to be working. She's coughing so hard her ribs are bruised. This is a walking pneumonia and she is still working. She went in for pain in the ribs a couple of days ago, and after x-rays and a CT scan, she still had pneumonia "unspecified", but now she also has thrush on her tongue... they gave her a different medication and sent her home. I'm wondering if she has this pneumonia, although she doesn't fit the age range. I hate that we don't know, and that clinics, public health, countries and media are not saying much. We're left to speculate and figure it all out on our own. We're living in scary times
The rapid antigen tests are a serious problem. I went to urgent care in late July with a fever of 105 F after having been sick a week and a half. The nurse at urgent care used the BinaxNow rapid antigen test to rule-out COVID. I suppose the fact that I had been sick for a week made the test a little more trustworthy, but I don't think urgent cares and ERs should be using these misleading tests. EDIT: I didn't have COVID, so the rapid test was correct, but I think they should use the PCR tests. They need to be made affordable if that is the problem.)
Somebody on reddit suggested that perhaps the 4-5 day delay is a result of our immune systems reacting sooner to the infection due to the virus no longer being novel. In other words, maybe the incubation period has been shortened by 4-5 days and the tests are performing no differently.
I have a whole pile of those rapid antigen tests, but I don't know what to do with them. They are so untrustworthy. All they do is give a false sense of confidence to people.