



HV.1, with Many Delta Variant Mutations is the Fastest Spreading Variant in the U.S./ BA.2.86 is Continuing to Spread at a Faster Pace & Could Become a Significant Challenge into Nov.
Unmitigated transmission also means faster evolution around treatments, vaccines and our immune response. We review asymptomatic risk. Outpatient visits and hospitalizations in children are increasing

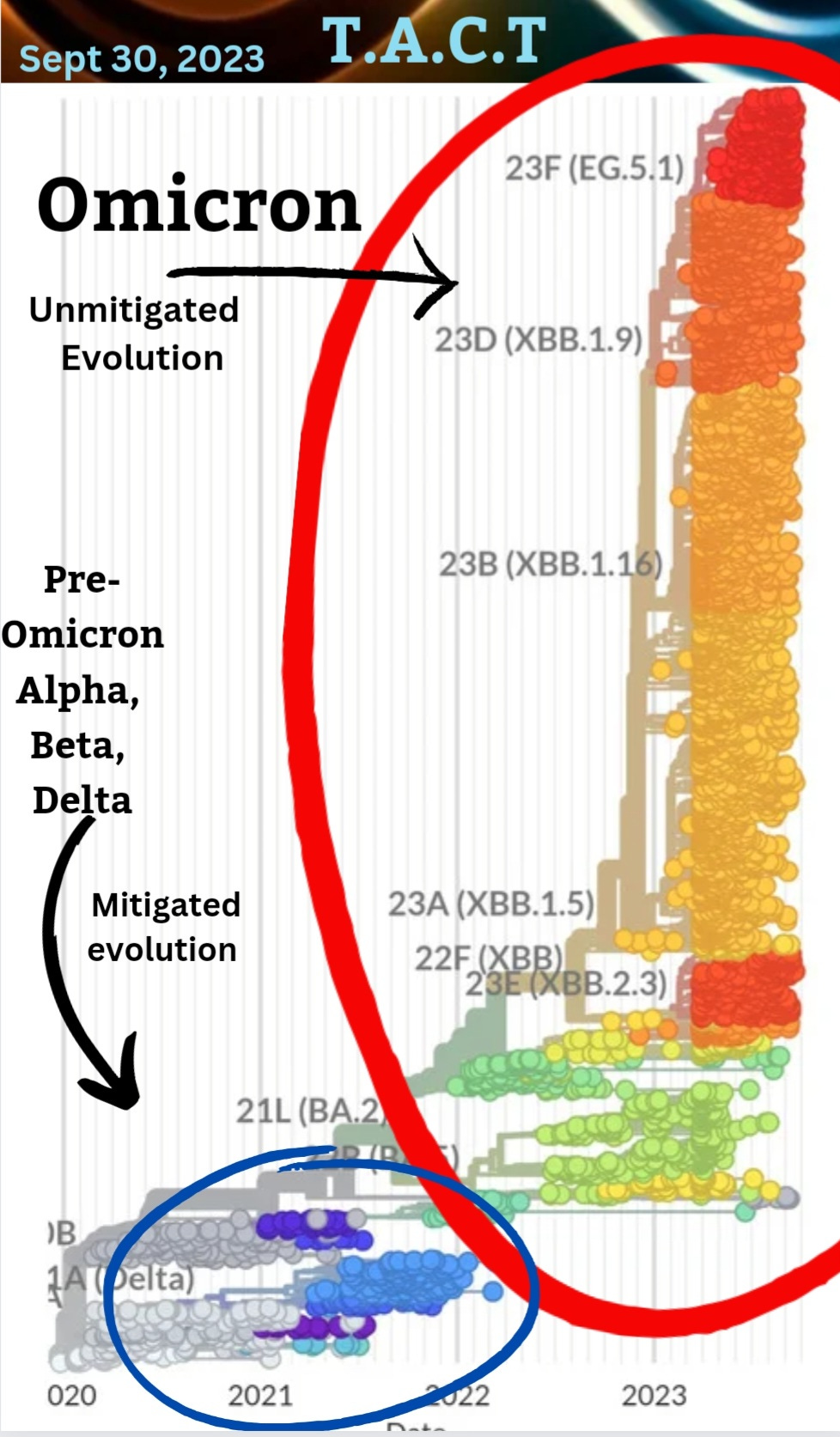
The difference between mitigating transmission or not is not only measured in lives lost & the millions suffering with long-term symptoms, & persistent infections, it is also measured in how fast COVID evolves, increasing the odds of variants capable of evading the latest treatments, vaccines and our own immune response. When we look at the picture below, we can see that COVID is more prevalent and has more paths to become more dangerous than ever before. New variants are continuing to spread around the globe within a couple months and are still causing surges of new cases, hospitalizations, Long-COVID, and death. By definition, COVID is not endemic. We are very much in the middle of a pandemic.
COVID is destroying the quality of life & ending the lives of more people with each new variant & we are allowing it to happen.
Long COVID (PASC)
A new study published in Sept 2023, reviews “studies that have identified SARS-CoV-2 RNA/protein or immune responses indicative of a SARS-CoV-2 reservoir in PASC samples. Mechanisms by which a SARS-CoV-2 reservoir may contribute to PASC pathology, including coagulation, microbiome and neuroimmune abnormalities, are delineated. We identify research priorities to guide the further study of a SARS-CoV-2 reservoir in PASC, with the goal that clinical trials of antivirals or other therapeutics with potential to clear a SARS-CoV-2 reservoir are accelerated.”
By becoming a paid subscriber, you're not only gaining access to exclusive content but also actively supporting the future of this important work. Contribute to our mission by becoming a valued paid subscriber today.
.
BA.2.86 (Pirola)
A study published on Sept 7th says, "The sera obtained from individuals vaccinated with 3rd-dose monovalent, 4th-dose monovalent, BA.1 bivalent, and BA.5 bivalent mRNA vaccines exhibited very little or no antiviral effects against BA.2.86. Moreover, the three monoclonal antibodies (Bebtelovimab, Sotrovimab and Cilgavimab), which worked against the parental BA.2, did not exhibit antiviral effects against BA.2.86. These results suggest that BA.2.86 is one of the most highly immune evasive variants ever."
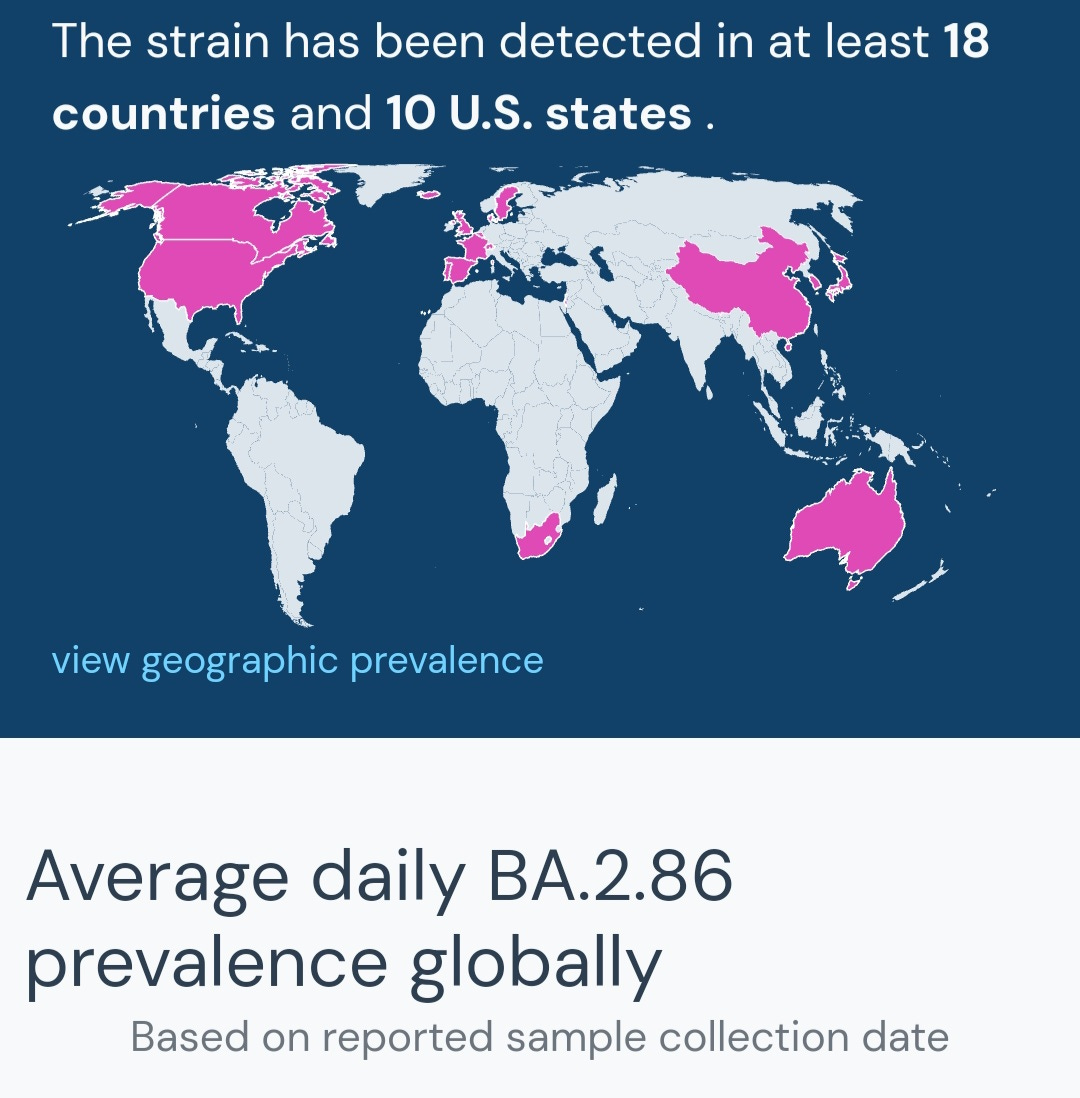
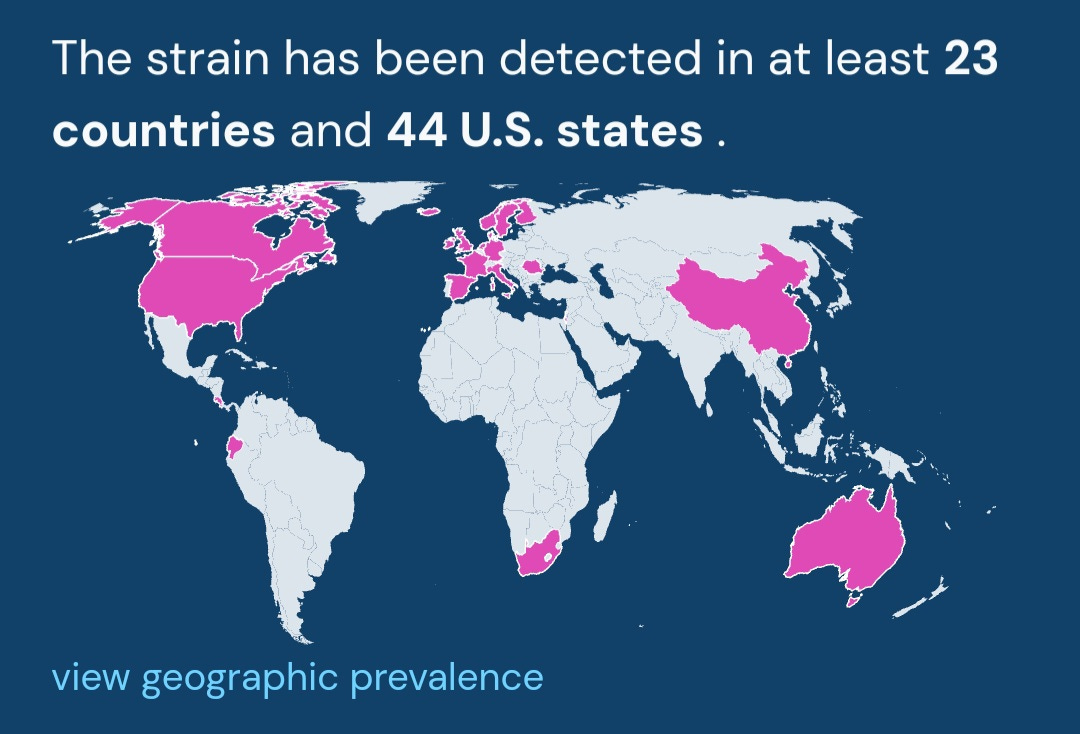
BA.2.86 (Pirola) continues to expand its footprint around the world, increasing the odds of adding even more mutations than it already has.
A study published on Sept 18, 2023, says “These findings suggest that BA.2.86 potentially has greater fitness than current circulating XBB variants including EG.5.1."
BA.2.86 is antigenically distinct from XBB.1.5, so how will that impact XBB.1.5 targeted vaccines?
BA.2.86 prevalence is still quite low but it is here and it is spreading at a faster pace. All of this data points to it having a very real chance of becoming a serious problem going into November and December. BA.2.86 isn't the only variant we have to worry about.
HV.1
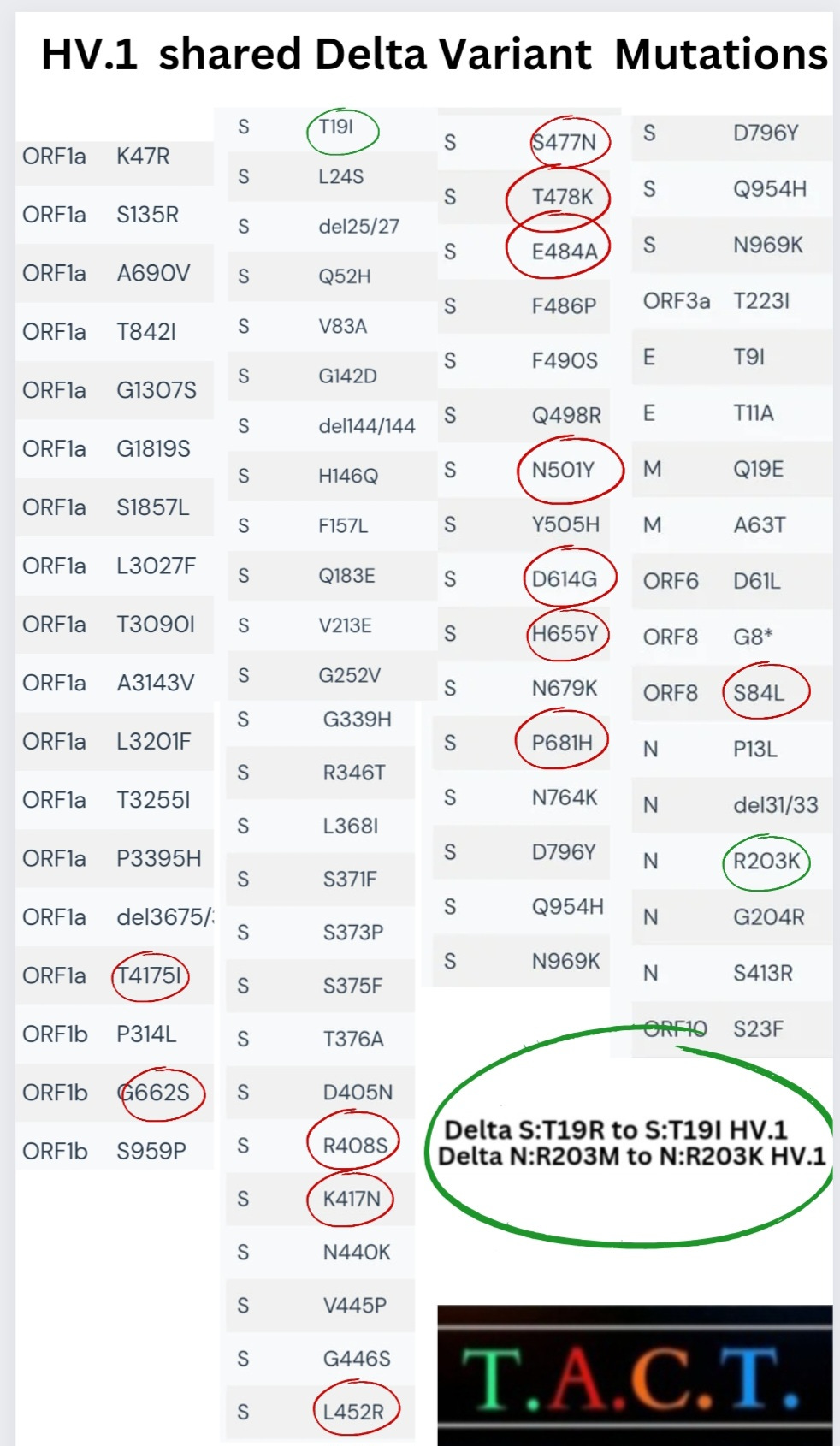
HV.1 has 13 of the same mutations as the more severe Delta variant. It was capable of ruining people's sense of taste & smell for months. In some cases, it is permanently altered. If taking our sense of smell and taste isn’t nightmarish enough, COVID can also infect our ears, leading to hearing loss. “Direct SARS-CoV-2 infection of the human inner ear may underlie COVID-19-associated audiovestibular dysfunction”
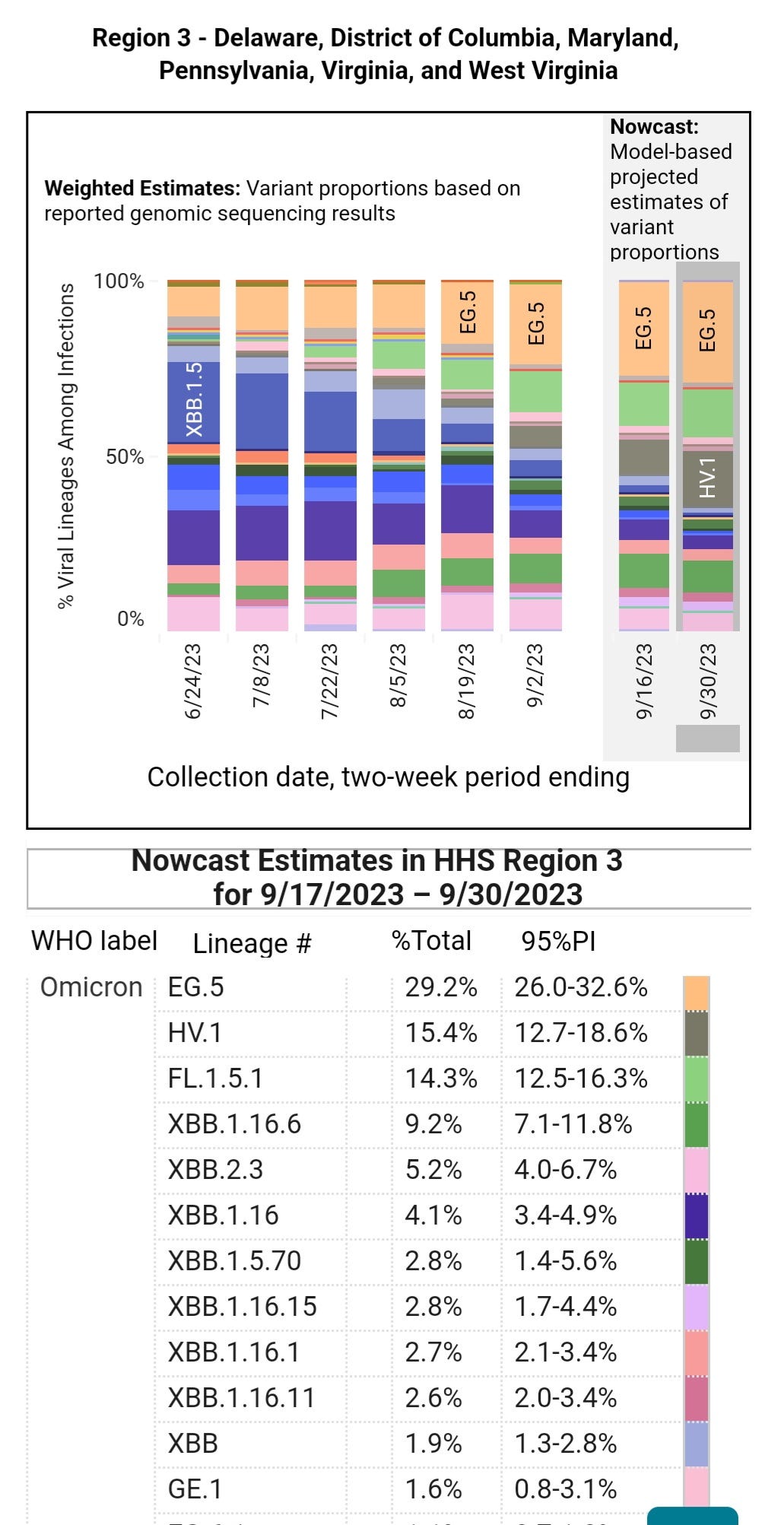
HV.1 is the fastest spreading variant in the U.S.
It has moved to the 2nd place spot in region 3, PA, VA, WVA, MD, DE & district of Columbia.
HV.1 is a highly evolved variant from the old Delta variant, with many of the most immune evasive/suppressive mutations of the XBB variants, making it even more concerning. We have little understanding of the short - or long-term implications of being infected with this variant.
Asymptomatic COVID Infections
(COVID without any symptoms and the potential repercussions)
Even without symptoms, the risk is real.
“Long-Term Consequences of Asymptomatic COVID Infection”
“Our results suggested that there were long-term effects of asymptomatic SARS-CoV-2 infection, such as loss of taste or smell, fatigue, cough, and so on."
Asymptomatic SARS-COV-2 infection has been found to persist in children's tonsils and adenoids. Children need these vital organs to help build a strong immune system. Having a persistent infection will cause untold levels of damage while aiding the virus in spreading for a longer duration.
We talk about the length of isolation from the start of symptoms quite often, and point out how the CDC guidance of 5 days isolation doesn't follow the science.
This study is just one more example of the negligence, particularly because we have known the infectious period lasts for a minimum of 8 days and as long as 20+ days, even without symptoms, since 2020.
"Asymptomatic individuals had median virus persistence duration of 8.87 days and 95 percentile duration of 20 days" was published in June 2020. This study recommended home isolation duration for COVID infected individuals in India should be extended from 17 days to at least 3 weeks "regardless of symptom status.”
Politics, not science, decided the CDC's negligent guidance of a 5-day isolation period and it has profound consequences.
Miscarriages may be caused by asymptomatic COVID infections.
The CDC guidance is responsible for many deaths & hospitalizations. The CDC guidance, says people should isolate for only 5 days before returning to work or school, sending people back while extremely contagious. They are ignoring the science and data. It's criminal negligence.
U.S. Outpatient Visits for Respiratory Illness by Age Group

We can see that children outpatient visits are increasing more than other age groups. Children under four are at the greatest risk because they have the least developed immune systems. School age children are getting infected and spreading the virus. Throughout the pandemic, children always increase first, followed by their parents age groups and then older adults because COVID spreads through schools and homes. Spreading from students to sibling. The siblings take it to new classrooms, infecting another classroom full of students. Parents and other caregivers get infected along the way.
Hospitalizations of Children are Increasing in England
Hospitalizations of children between 6-17 years old have increased +37.5%

This is predictable, and importantly, this is preventable.
We must work Together Against COVID Transmission.
tActNow.info/clean-air-for-kids.com
#CovidIsNotOver
Hi TACT...
Thought I would throw this reference onto the pile if you haven't seen it.
Grape Seed Extract seems like an inexpensive, potentially useful, supplement that might be beneficial in creating a hostile environment for SARS-CoV-2.
https://elifesciences.org/articles/84899#:~:text=The%20study%20reports%20new%20findings,SARS%2DCoV%2D2%20infection
I'm a teacher, and school started at the beginning of September. I already have had several students out multiple times, for days at a time because of "allergies", "colds", and the "flu". They all test one time, it's negative, and then they come back, still with symptoms, but no longer any fever. It's so out of the norm for this time of year, yet no one is batting an eye.