



Novavax Cleared FDA and CDC Approval, but There are Still Unanswered Questions
How effective will the updated vaccines be against the highly mutated JN.1 variant?

The newly approved 2023 COVID-19 vaccines are formulated to target XBB.1.5, which was dominant in early 2023 when public health officials made the reformulation decisions. We have a situation in which COVID is evolving at an extraordinary pace. This rapid evolution is due to the unmitigated transmission reaching more people, including immunocompromised people that had protected all of us by protecting themselves from the increased likelihood of the virus surviving longer in their bodies thus having more time to evolve around treatments and vaccines.
We have failed to protect the most at risk people and that in turn is aiding in the viruses evolution. COVID has an evolutionary advantage over us as long as we allow it to spread at the rate it is spreading.
Research and observations from trials, such as those for HIV, malaria, and the Pertussis vaccine, have indicated that repeated vaccinations can lead to reduced protection from infection. A consistently overlooked point is on the timing of vaccination after a prior dose and/or after an infection and what could happen if infected in the months after receiving a COVID vaccine. How does the immune system respond?
Importantly, will the XBB.1.5 targeted vaccines provide any benefit and if so, for how long? Lastly, how well will it work against what is looking to be the next dominant variant, JN.1 (BA.2.86.1.1)? JN.1 is a sub-variant of the BA.2.86 (Pirola) variant.
In order to discern these questions, we need additional data. We have not seen the following data from Pfizer, Moderna or Novavax. If someone reading this knows where to find this data then please share a link to that information in the comments.
1. lgG4/lgG1 ratio at 3,6,& 9 months.
2. Spike specific T-cells response at 1,2, and 3 months post vaccination.
3. Memory CD8 T-cell response at 3,6, & 9 months post vaccination.
4. Efficacy against the JN.1 variant or its parent, the BA.2.86 variant.
So far, most data shows the JN.1 variant may be able to evade an XBB.1.5 targeted immune response. A pre-print study from early Sept. says, “BA.2.86 significantly evades convalescent plasma from XBB breakthrough infection (BTI) and reinfections.”
”In sum, we found that BA.2.86 is antigenically distinct from XBB.1.5 and can escape XBB-induced neutralizing antibodies. The updated vaccine's efficacy against BA.2.86 should be closely monitored.”
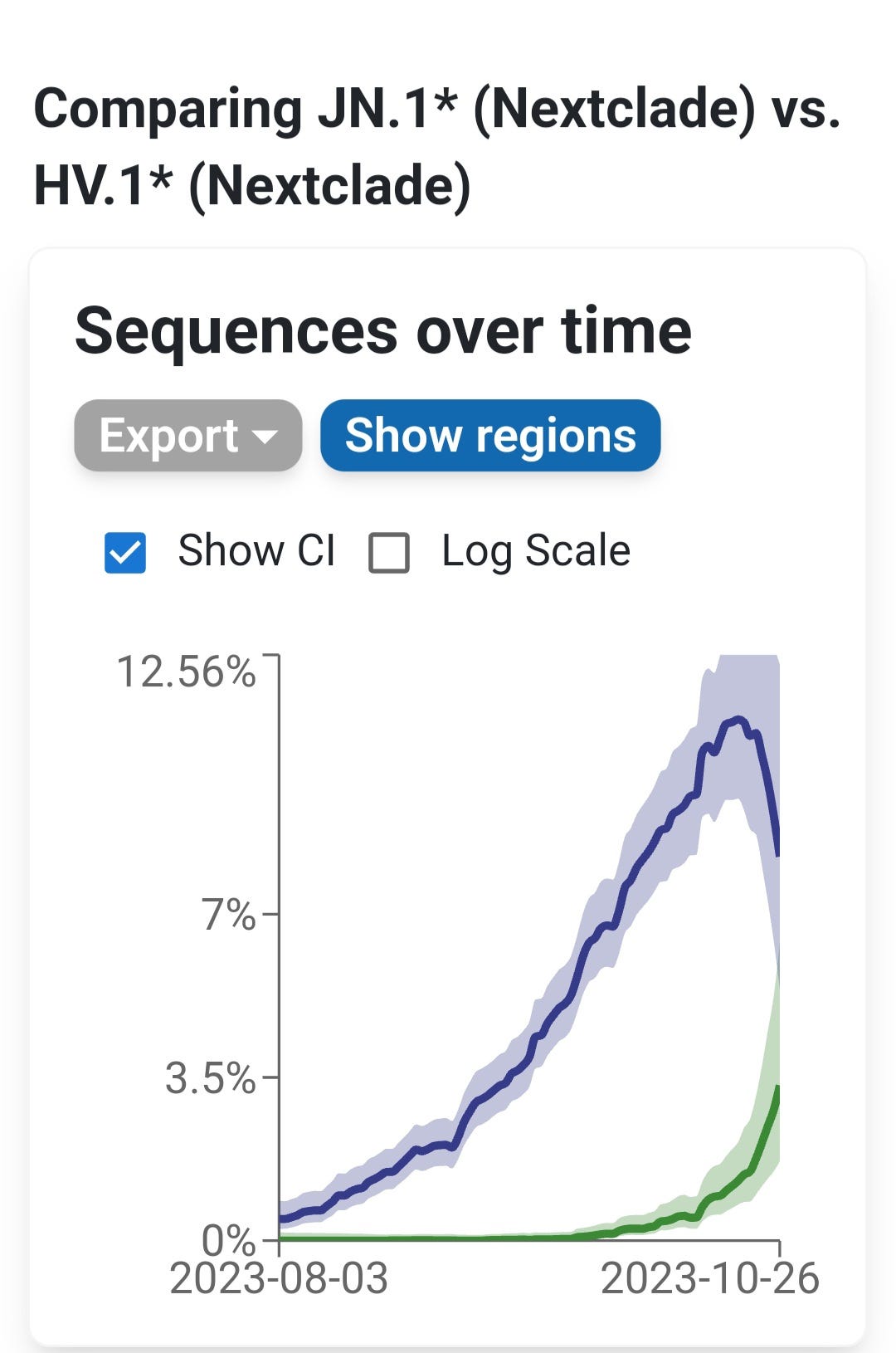
The trajectory of JN.1 (BA.2.86.1.1) expansion has it becoming a significant percentage of cases by sometime in late November to mid-December, if it keeps spreading as it is now. We can see below that HV.1 (blue line), the current dominant variant in the U.S. is starting to decline while JN.1 (green line) is growing at an exponential rate.
Novavax Oct 3, 2023 Update Leaves More Questions than Answers
Novavax added a line to their Oct 3, 2023 statement saying it has efficacy against BA.2.86 but the references provided by Novavax to support the statement do not discuss the updated XBB.1.5 vaccine. Reference 1 is from 2022 so that obviously doens’t reflect on how the new XBB.1.5 targeted vaccine is impacted by BA.2.86 or JN.1 (BA.2.86.1.1) Reference 2 discusses COVID evolution and doesn’t mention Novavax so if anyone has additional sources or explanations as to how these are valid sources showing that the latest Novavax, XBB.1.5 targeted vaccines efficacy against the BA.2.86 variant or its sub-variants, please share that information. The Novavax statement says the following;
"The EUA was based on non-clinical data showing that Novavax's COVID-19 vaccine induced functional immune responses against XBB.1.5, XBB.1.16 and XBB.2.3 variants.”
Then they say, "Additional non-clinical data demonstrated that Novavax's vaccine induced neutralizing antibody responses to newly emerging subvariants BA.2.86, EG.5.1 FL.1.5.1 and XBB.1.16.6 as well as robust CD4+ polyfunctional cellular (T-cell) responses against EG.5.1 and XBB.1.16.6. These data indicate Novavax's vaccine can stimulate both arms of the immune system and may induce a broad response against currently circulating variants.1,2"
Note in the pic below from the Novavax, Oct 3rd update, they link references 3,4, and 5 but not 1 and 2. Why wouldn’t they want people to focus on that? (sarcasm)

For your convenience, the references are linked below.
1. - Note: This is from 2022? Wherry EJ, Barouch DH. T cell immunity to COVID-19 vaccines. Science. 2022;377(6608):821-822. doi:10.1126/science.add2897.
https://pubmed.ncbi.nlm.nih.gov/35981045/
2. Note: This doesn’t mention Novavax.
Markov PV, Ghafari M, Beer M, et al. The evolution of SARS-CoV-2. Nat Rev Microbiol. 2023;21(6):361-379. doi:10.1038/s41579-023-00878-2.
https://www.nature.com/articles/s41579-023-00878-2
The October 3rd update goes on to say, "In clinical trials, the most common adverse reactions associated with Novavax's prototype COVID-19 vaccine (NVX-CoV2373) included headache, nausea or vomiting, muscle pain, joint pain, injection site tenderness, injection site pain, fatigue and malaise."
John C. Jacobs, President and Chief Executive Officer, Novavax, said, "Novavax's authorization today means people will now have the choice of a protein-based non-MRNA option to help protect themselves against COVID-19, which is now the fourth leading cause of death in the U.S. In the coming days, individuals in the U.S. can go to pharmacies, physicians' offices, clinics and various government entities to receive an updated Novavax vaccine."
The link to the October 3, 2023 Novavax company statement:
https://ir.novavax.com/press-releases/2023-10-03-Novavax-2023-2024-COVID-19-Vaccine-Now-Authorized-and-Recommended-for-Use-in-the-U-S
The updated vaccine could hinder an effective immune response in two ways but having the data would help answer if these possibilities are valid concerns or not.
1. Existing XBB.1.5 targeted T-cells may be more easily evaded and/or infected, while the body tries to upgrade or replace the existing T-cell army with more capable T-cells to eliminate BA.2.86, an antigenically distinct variant from XBB.1.5. The process could cause excess cell loss, T-cell exhaustion, and excess cytokine release. Increased cytokine production, mainly IL-6 and/or IL-10 could cause mast cell activation which can produce more fibrin, leading to an increased odds of coagulation and blood clots, which is behind the inflammation and vascular dysfunction.
2. If too many lgG4 antibodies are created then that could get in the way of lgG1 and lgG3 antibodies from blocking the virus and from signaling other immune cells. lgG4 antibodies don't signal the rest of the immune system and are generally the least prevalent type of lgG antibody however if exposed to a large amount of an antigen then more are created by B-cells switching. An earlier study showed Novavax, along with mRNA vaccines, caused more lgG4 antibodies. This could make infection more likely after about 2 to 3 months from taking the vaccine. This is the likely reason Walgreens data showed boosted people were more likely than unvaccinated to be infected after 3 months. The Walgreens data showed this for over a year. Recently, they removed the graphic showing this. The likelihood of infection increased more as time went on. High levels of LgG4 antibodies and autoantibodies are implicated in quite a few autoimmune disorders so that's one more issue that can have, potentially, lifelong consequences. To read more on this:
Are you considering taking an updated vaccine? Are you concerned about the risks and potential for autoimmune reactions post-vaccination? You're not alone.

Are you considering taking an updated vaccine? Are you concerned about the risks and potential for autoimmune reactions post-vaccination? You're not alone. Similar concerns have arisen not only with mRNA vaccines but also with other vaccine types and after COVID infections.
Thank you for sharing this! I'm not sure whether to get Novavax due to this, also since it's $130 and I don't have insurance. I've been behind boosters because of all the conflicting info and how fast Covid has been mutating, but I want to protect myself with more than my N95 and air purifiers at home. This is so frustrating!
I got the Novavax vaccine after 4 doses of Moderna. I had zero side effects, which was a pleasant change. I don't have any worries about a possible autoimmune response. The effect of covid is what worries more.