



COVID Update: Uncharted Territory: Exploring the Surge of Infections Beyond Seasonal Norms and the Failure of the CDC's Vaccine Focused Approach
A deeper dive into the real-world consequences of reducing mitigation protections in the face of waning immunity and more immune evasive and suppressive variants.

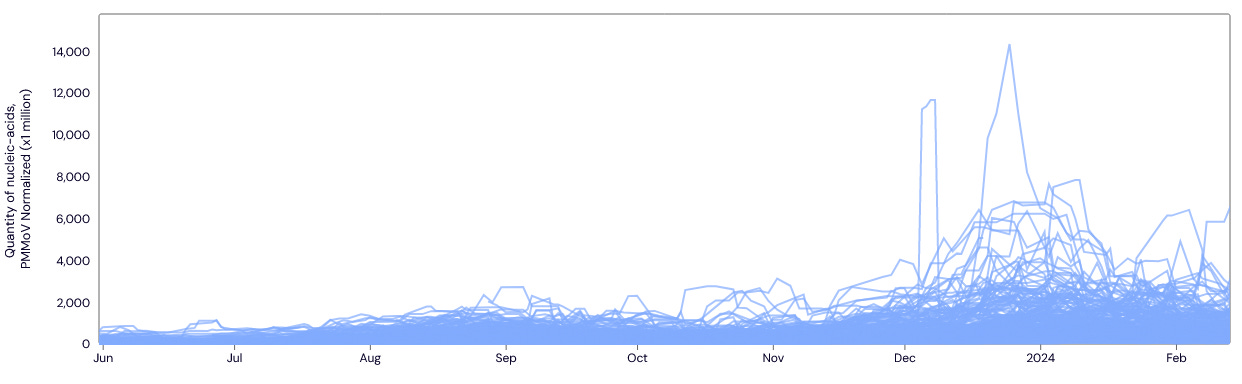
The relentless spread of JN.1 and its numerous sub-variants continues to inflict significant damage across the U.S. JN.1 emerged in November 2023. JN.1 and its offspring account for over 90% of all transmission. In the graph below, JN.1 is represented by the purple lines on the right side, illustrating its rapid rise to dominance.

The data from the two national wastewater reporting sites paints a concerning picture: overall prevalence of the virus remains high across the U.S., with many areas experiencing a rise in prevalence. The line graph below shows data from all the testing sites that wastewater scan reports and it’s clear that the amount of virus circulating is higher than at any time since April 2022.

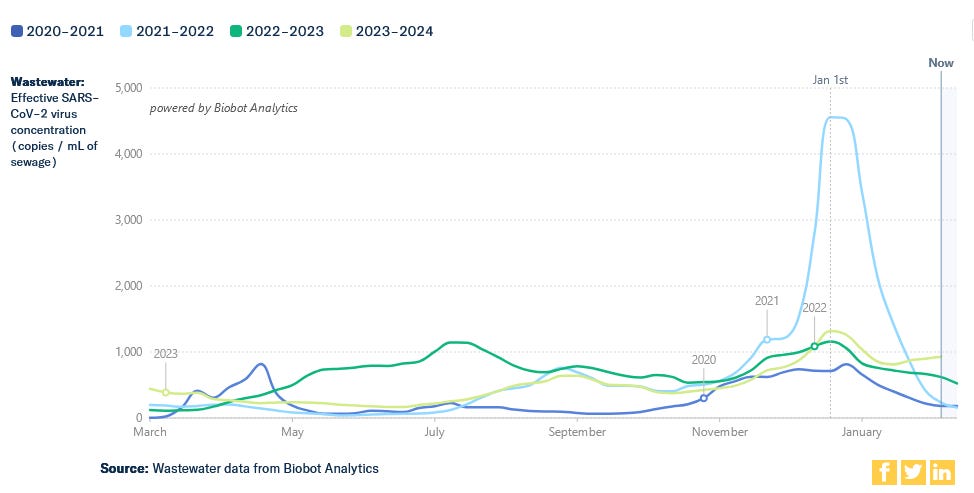
Upon closer examination, below, we observe that since November 2023, the prevalence of SARS-CoV-2 in wastewater reached its peak in late December or early January. Subsequently, it began to decline from the peak but leveled out swiftly thereafter. Currently, we are witnessing a very high baseline of transmission and an increasing prevalence in many locations.
If we look at the year-over-year from Biobot, we can see that even though they have different testing sites, their data is in agreement with what is shown above.
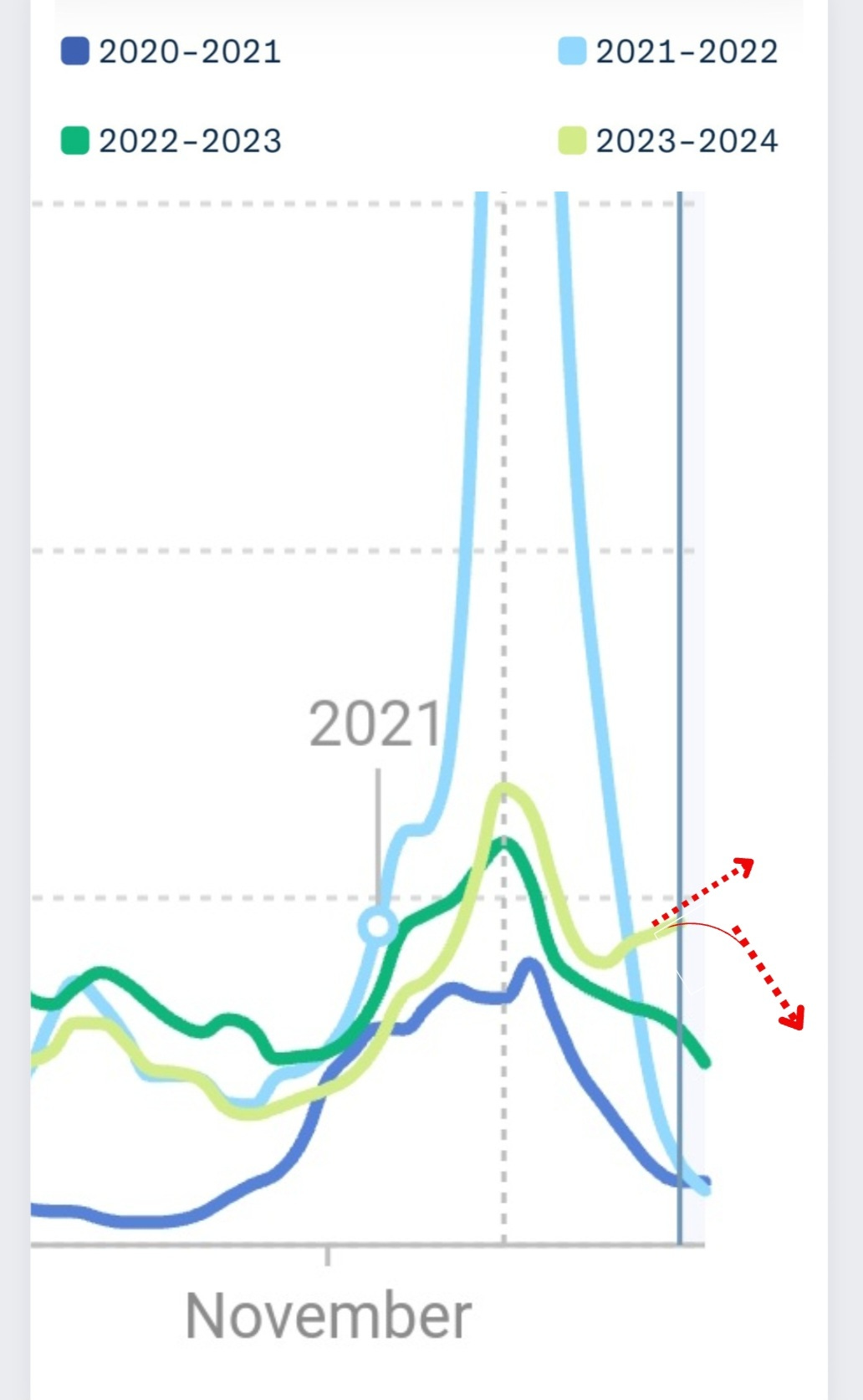
Zooming in for a closer look, below, it becomes evident that even if prevalence were to start declining, we would remain significantly above typical levels for this time of year for the next month or two. However, the concerning reality is that prevalence is actually on the rise in many areas, indicating that we are undeniably navigating uncharted territory.
Real-world Consequences
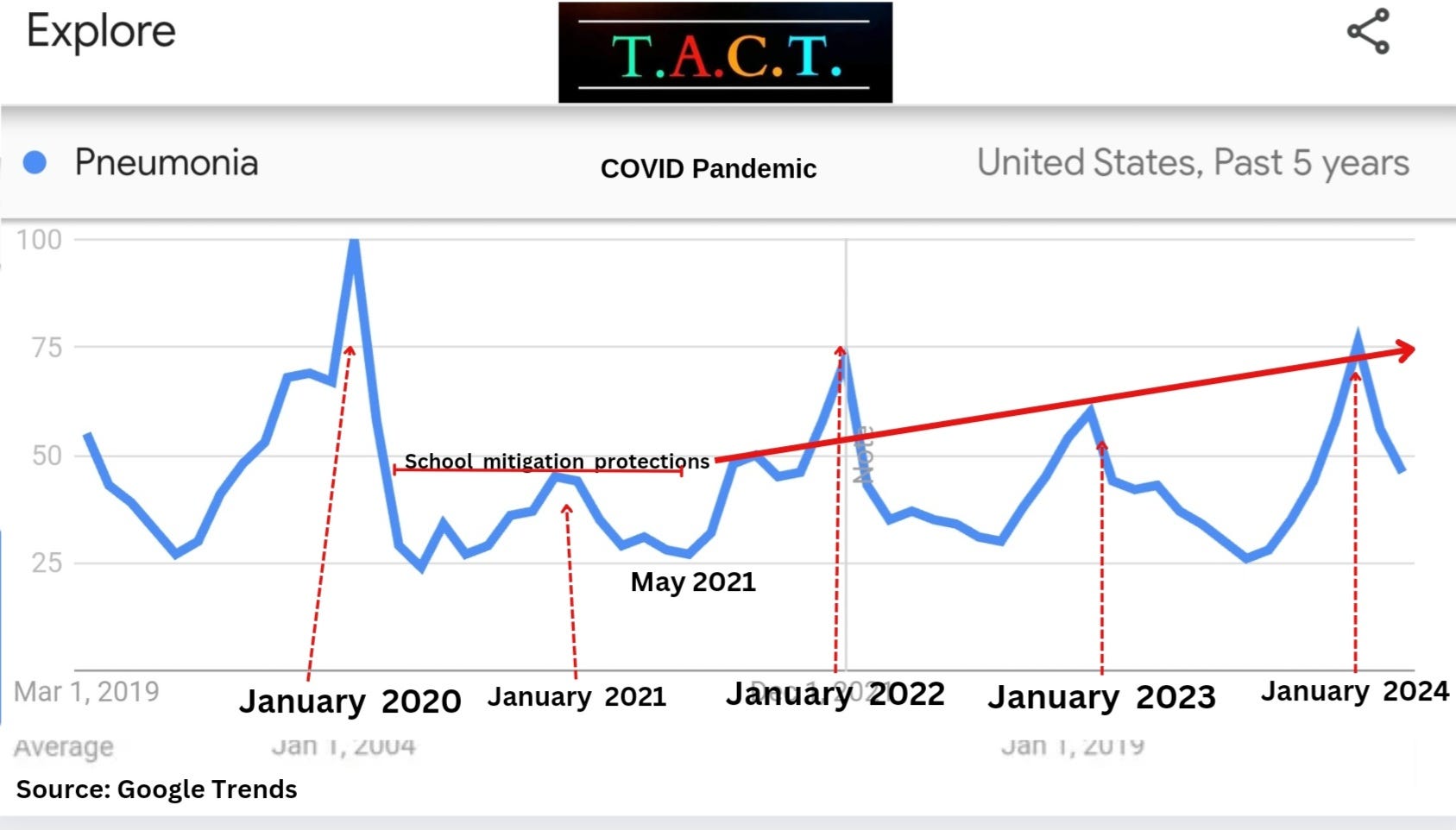
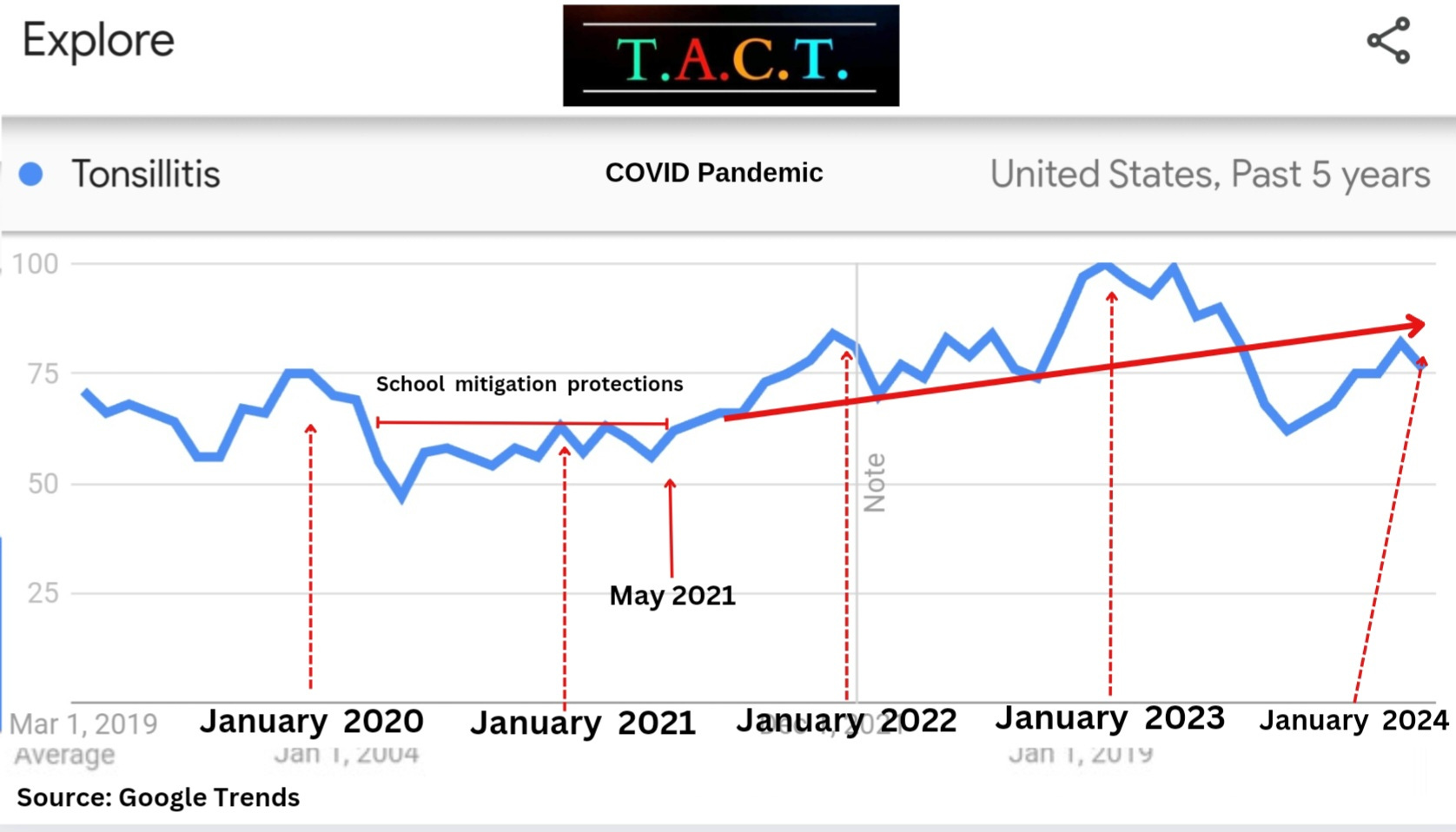
The graphs below, sourced from Google Trends, depict the frequency of searches for pneumonia and tonsillitis. It underscores quite a few crucial points.
The mitigation measures implemented in 2020 to curb the spread of airborne pathogens notably decreased illness levels.
The removal of these measures in May 2021 resulted in a significant surge in illnesses caused by airborne pathogens. The repercussions of disregarding scientific evidence and data, and failing to take action to prevent airborne transmission are profound. They include unnecessary and preventable hospitalizations, disability or reduced quality of life, increased healthcare expenses, lost wages and education, tens of thousands of deaths, and a reduction in life expectancy for many individuals.
COVID-19 Lung Damage
A study published January 25, 2024, looked into the lung function of individuals with mild COVID infections, 2 years after the initial infection. We don’t know if these people were reinfected in between but the end result is alarming. They concluded, “Our results indicate that mild COVID-19 infection affects lung function at the time of infection with limited recovery 2 years after infection.”
Can COVID-19 damage children's lungs?
Yes, COVID-19 can lead to widespread functional lung alterations in children and adolescents. "Low-field-strength MRI showed persistent pulmonary dysfunction in children and adolescents who recovered from COVID-19 and those with long COVID."
Babies are being born with smaller lungs, increasing the risk of viruses like RSV and flu, with an array of potential issues in the future.
COVID-19 Infection and Persistence in Tonsils and Adenoids
Is there evidence showing that COVID-19 can persist in children’s tonsils and adenoids even if they didn’t have any symptoms during the acute phase of the infection?
Yes. Tonsils and adenoids are major sites of persistent COVID infections in children without any symptoms. The tonsils and adenoids are important for the development of the immune system. We don’t know how many kids this is impacting or how many more it will impact. This study also suggests that persistent infections in the tonsils may play an important role in community transmission. “Lymphoid tissue can be a reservoir of SARS-CoV-2 and may play an important role in community dissemination.”
We must ascertain the number of children who underwent tonsil or adenoid removal due to persistent COVID-19 infections. These organs are vital for bolstering the immune system during childhood. When children endure recurring infections or require surgical intervention, it adds additional layers to the long-term damage inflicted on their immune systems. This damage could be costing children and adults decades of their lives and reducing their quality of life at a much earlier age.
Each year follows a similar pattern: illness escalates from October through late December/early January, then gradually subsides until this year which remains high. January 2021 stood out as an exception to the surge. Why? Because we prioritized the prevention of airborne transmission, particularly important in schools.
Why did searches for pneumonia, tonsillitis, pink eye, and many other health problems start increasing in May of 2021 and largely remain high until now?
In May 2021, despite having clear indications that the vaccines wouldn't halt transmission, persistent infections, Long COVID, or COVID's evolution, the CDC revised its guidelines to permit increased transmission. At that time, Walensky, the CDC director, declared, “Anyone who is fully vaccinated can participate in indoor and outdoor activities, large or small, without wearing a mask or physical distancing. If you are fully vaccinated, you can start doing the things that you had stopped doing because of the pandemic. We have all longed for this moment when we can get back to some sense of normalcy.”
This misleading statement relieved the burden carried by many conscientious individuals who prioritized protecting themselves and others. Its repercussions persist, lingering in the minds of vaccine recipients, despite years of mounting evidence showing that immunity wanes and the reduced risk of infection is very short-lived (less than 3 months). We also have many studies showing the risks of asymptomatic or mild infections so the continued drive to rewrite the guidance, allowing more transmission goes against all the science and data.
How could the CDC know that the vaccines had short-lived efficacy in preventing infections?
Here is a chronological list of studies indicating that they should have been aware. Even if they weren't initially, the continuous stream of studies showing the waning efficacy of the vaccines would have brought it to their attention at some point. So, why haven't they reversed course to bolster mitigation measures, especially considering the evidence that the vaccines didn't offer long-term protection against infections and the declining uptake of boosters over time?
(May 17, 2021) "Modeling of the decay of the neutralization titer over the first 250 days after immunization predicts that a significant loss in protection from SARS-CoV-2 infection will occur, although protection from severe disease should be largely retained. Neutralization titers against some SARS-CoV-2 variants of concern are reduced compared with the vaccine strain, and our model predicts the relationship between neutralization and efficacy against viral variants." (Published in Nature Medicine, May 17, 2021)
(August 11, 2021) "BNT162b2 effectiveness against any Delta infection, symptomatic or asymptomatic, was 64.2% ≥14 days after the first dose and before the second dose, but was only 53.5% ≥14 days after the second dose, in a population in which a large proportion of fully vaccinated persons received their second dose several months earlier."
"Both BNT162b2 and mRNA-1273 are highly effective in preventing Delta hospitalization and death, but less so in preventing infection, particularly for BNT162b2." (Pre-print published August 11, 2021 )
(Published in Nature Medicine November 2, 2021)(September 7, 2021) "Taken together, these data constitute an early signal for waning protection against symptomatic illness"
(pre-print published Sept 7, 2021)
(published in PNAS nexus, June 8, 2022)(December 9, 2021) "Conclusions: These findings indicate that immunity against the delta variant of SARS-CoV-2 waned in all age groups a few months after receipt of the second dose of vaccine." ( published in New England Journal of Medicine December 9, 2021)
(March 10, 2022) "Waning protection against infection over time was due to both declining immunity and the emergence of the delta variant." (Published March 10, 2022)
(April 2022) "Vaccine effectiveness waned after the second dose: at 5 months, BNT162b2 effectiveness was 82·1%" (published April 2022)
(October 21, 2022) "3rd dose monovalent efficacy against hospitalization decreased to just 29% after 120 days. That was against BA.5. It's going to be much lower against future variants. Three-dose VE during the BA.1/BA.2 and BA.4/BA.5 periods was 79% and 60%, respectively, during the initial 120 days after the third dose and decreased to 41% and 29%, respectively, after 120 days from vaccination."
(Published by the CDC/MMWR)
The list of studies highlighting the limited effectiveness of the vaccines continues to grow, with their efficacy declining over time. Despite a substantial body of evidence indicating that the vaccines do not fully prevent infections, Long COVID, or the evolution of COVID, the CDC persists in advocating for a vaccine-only approach.
They overlook the fact that less than 20% of the population has received an XBB.1.5 targeted vaccine. Moreover, they disregard numerous studies demonstrating the limited short-term benefits of the XBB.1.5 targeted vaccine
Despite being aware of these facts, the CDC continued on a course reducing protections for the population and is still attempting to further reduce the mitigation protection measures. Consequently, thousands of lives are lost each week, and millions suffer from Long COVID. Countless families find themselves caring for sick children or unable to work due to illness.
This outcome was foreseeable and is entirely preventable. The CDC's failure to offer comprehensive guidance focused on preventing infections places our children at risk of economic instability and long-term health complications that will greatly diminish their quality of life and, ultimately, shorten their lifespans. Decisive leadership is urgently needed to implement the necessary changes and steer us away from this unsustainable trajectory.
"Compared to a waned third dose, fourth dose VE was 13.1% (95% CI 0.9 to 23.8) overall; 24.0% (95% CI 8.5 to 36.8) in the first 2 months post-vaccination, reducing to 10.3% (95% CI −11.4 to 27.8) and 1.7% (95% CI −17.0 to 17.4) at 2–4 and 4–6 months, respectively."
"Relative to an infection >2 years ago and controlling for vaccination, 63.6% (95% CI 46.9 to 75.0) and 29.1% (95% CI 3.8 to 43.1) greater protection against infection was estimated for an infection within the past 0–6, and 6–12 months, respectively."
(Published:December 13, 2023)
https://www.thelancet.com/journals/lanepe/article/PIIS2666-7762(23)00228-4/fulltext
There are about 100,000 schools in the US. I think $10,000/year per school would cover the cost of buying and operating one HEPA H13 air purifier per classroom. That would be $1 billion per year for the US. That's a lot of money, but it might help.
More sensitive home test kits would be a huge help. The false negatives aren't helpful.