



COVID Update: 4/20/2023 Exponential Growth Continues in India and Singapore. The Rise of the Next Generation of Variants. COVID Pneumonia's Impact
Why Ending the Universal Use of Masks in Hospitals is a Huge Mistake

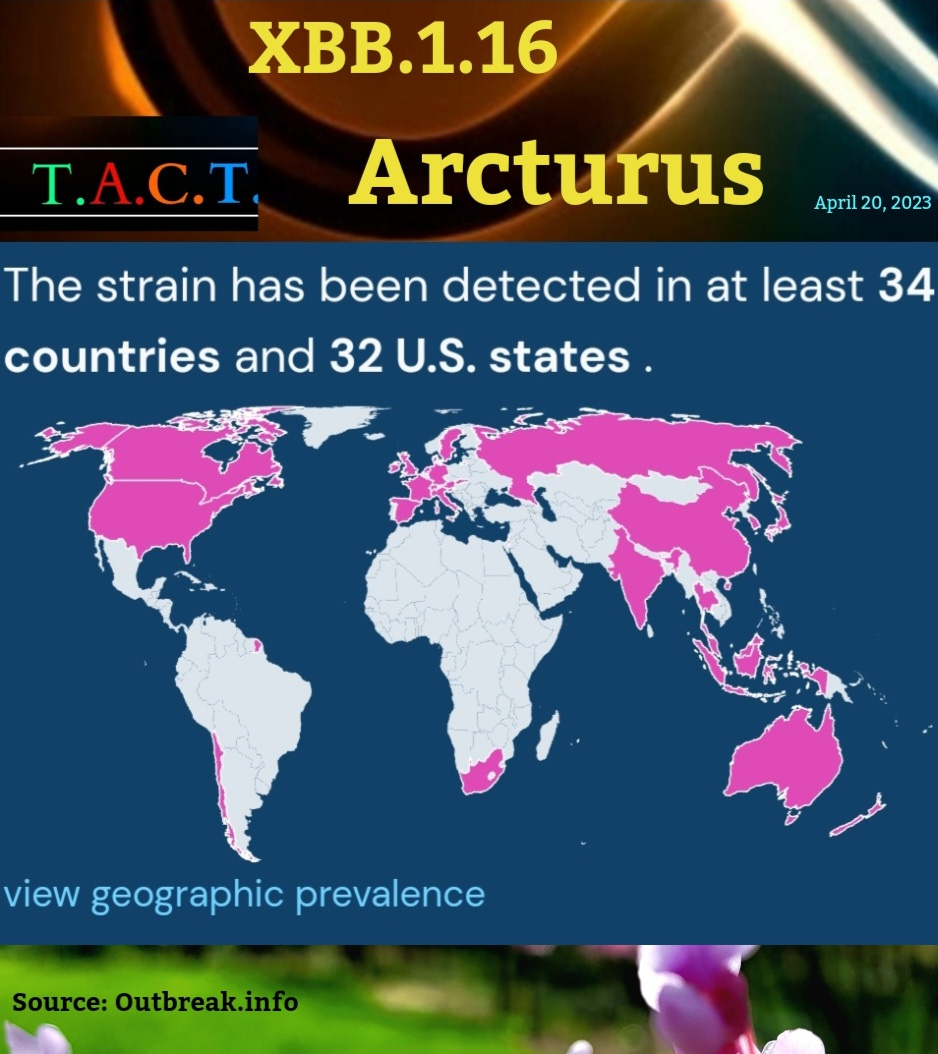
XBB.1.16 has spread to at least 34 countries and 32 U.S. states.
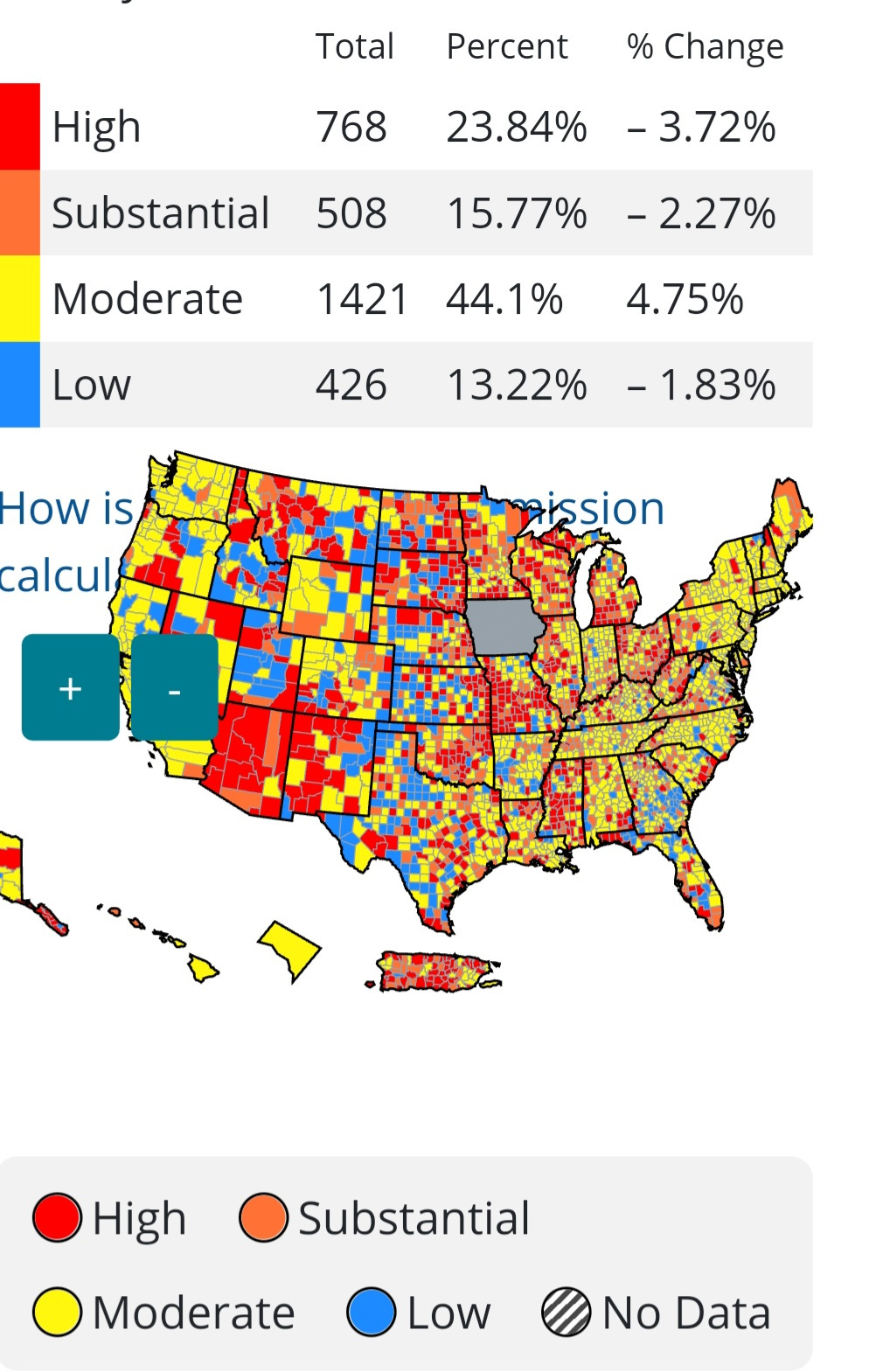
The United States is watching its surveillance system collapse to a bare minimum that isn’t adequate given the direction of COVIDs evolution. Iowa stopped reporting COVID data and Florida is in question at the moment. Based on what the CDC is showing, with very low rate of recorded tests, only 13% of the U.S. is in low transmission. 39% is in Substantial or High Transmission and 44% is Moderate.
Ending the Universal Use of Masks in Hospitals is a Huge Mistake
A small group of infectious disease doctors published an opinion piece that is getting some media coverage. They are calling for masks to be removed in healthcare settings, but they are completely ignoring the risks that COVID poses to patients. Removing universal mask use will ensure more immunocompromised become infected with more than one variant, increasing the odds of new recombinant variants that are better equipped to evade the latest treatments and our immune system.
The Rise of the Next Generation of Variants
The virus responsible for COVID-19 is evolving rapidly, with mutations occurring frequently in its body. This suggests that the virus is trying to overcome our strong T-cell defense. There is evidence that the latest generations of variants, with mutations that could possibly affect the T-cell response, are causing an increase in hospitalizations and deaths in India and Singapore.
A case that was sequenced in India on March 14th, known as the XBB.1.16.1 variant, has several mutations that may be contributing to this rise. N:L64Q, N:K65N, N:S78R, N:S79C, ORF8:D34N, S:T346R, S:N477S, S:S486F. These mutations may be able to weaken our T-cell response, which is our last line of defense against the virus. If the virus can get past our T-cell defense, there is a higher likelihood of persistent infections, chronic conditions, and increased mortality rates, even among younger people. Therefore, this situation should be of great concern to all of us.

COVID Pneumonia
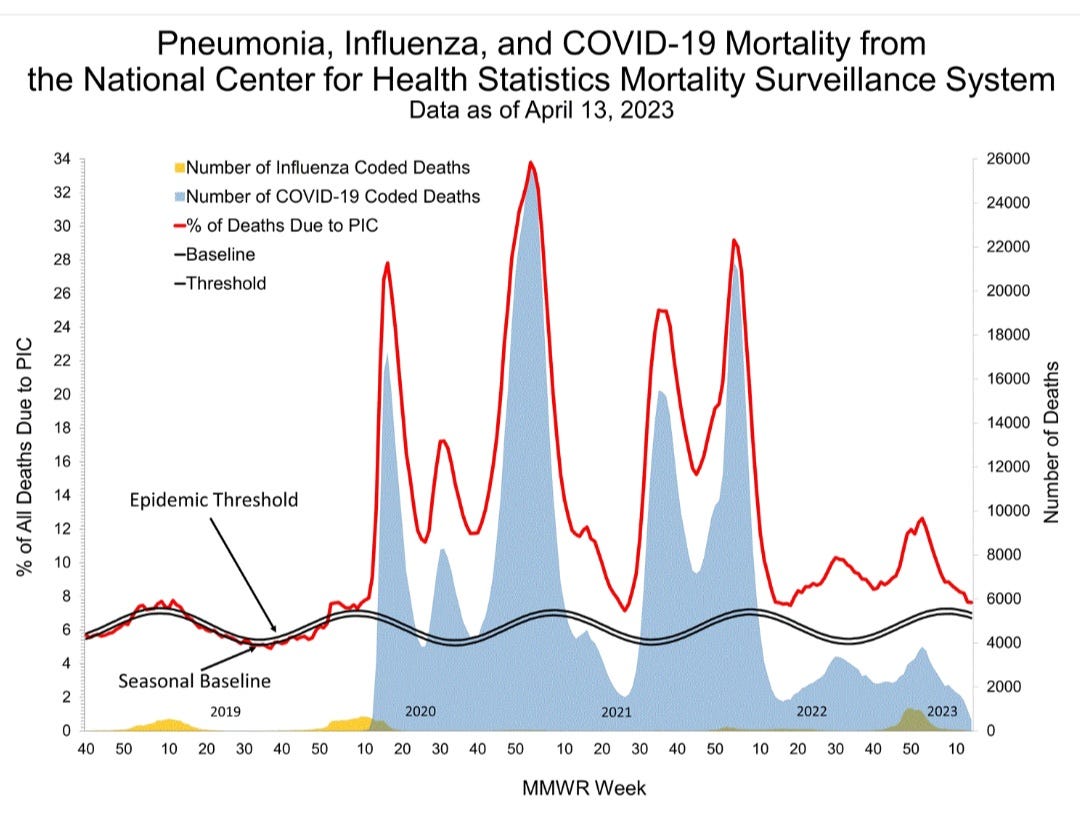
Looking at the graph below we can see that the deaths from Pneumonia, Influenza and COVID are still above the Epidemic threshold. COVID Pneumonia is very likely, not being recorded as COVID deaths in a large number of patients. Pneumonia is killing more people than COVID and Flu combined right now. The reason it isn’t recorded is because by the time people go to the hospital the PCR tests are coming back negative. They are missing the fact that COVID can persist in the tonsils, adenoids, and lungs long after the initial infection and that isn’t showing up on the PCR tests.
Pulmonary fibrosis can be a manifestation of asymptomatic or mild COVID. This study, published May 2022, said, "On evaluation, after excluding other causes, the fibrosis was attributed to asymptomatic or mild COVID illness in the past." They note that there is no definitive treatment for post-COVID fibrosis of the lungs.
What does COVID do to lungs?
COVID-19 can cause lung complications such as pneumonia and, in the most severe cases, acute respiratory distress syndrome, or ARDS. Sepsis is another possible complication of COVID-19 which can also cause lasting harm to the lungs and other organs.
This study published in November 2022, “Increase of mast cells in COVID‐19 pneumonia may contribute to pulmonary fibrosis and thrombosis”, noted a significant increase of mast cells in SARS‐CoV‐2‐infected lung tissue compared to influenza.
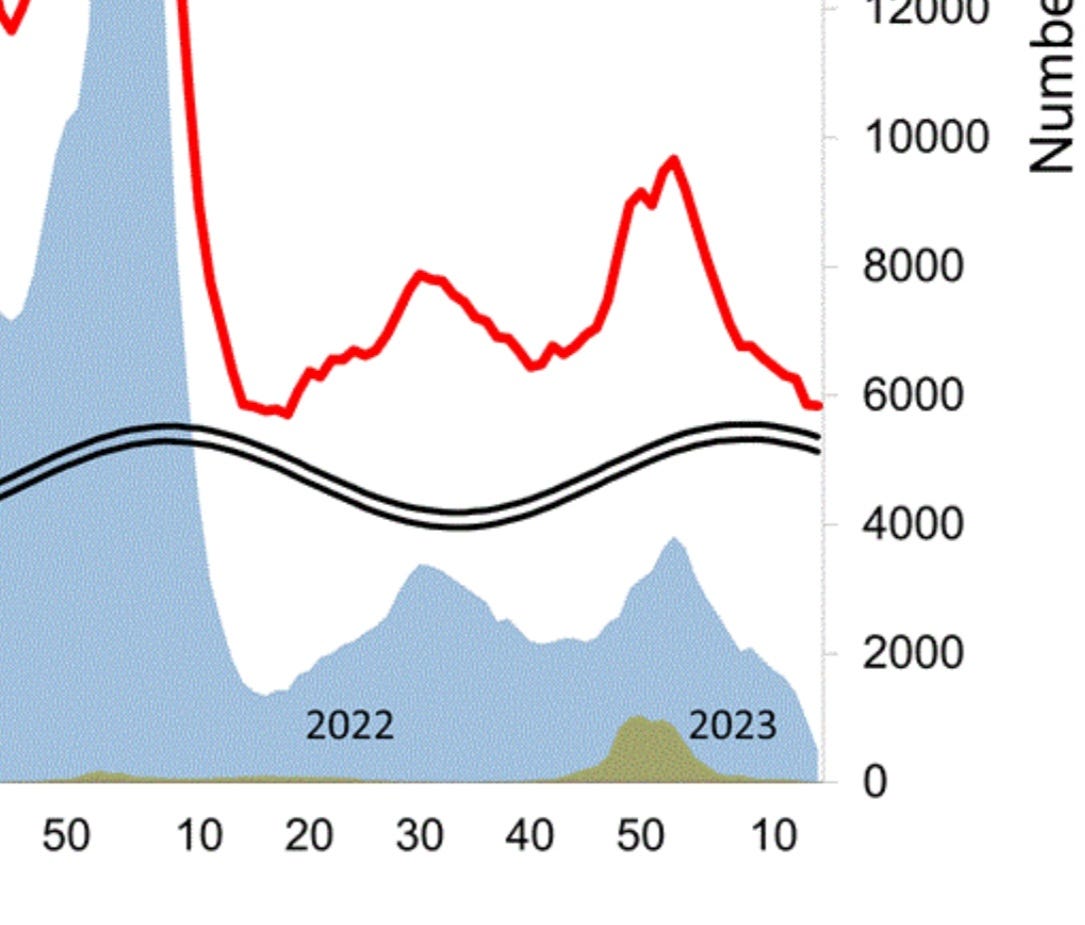
Zooming in below, we see that despite low deaths from COVID and Flu, Pneumonia is keeping the amount of deaths above the threshold. Deaths from pneumonia, flu, and COVID are still above the pre pandemic baseline and will very likely start increasing again with the latest variants and the removal of masks in hospitals. Removing universal mask use will ensure that more people suffer and die. COVID is likely leading to many more pneumonia deaths than are actually being acknowledged.
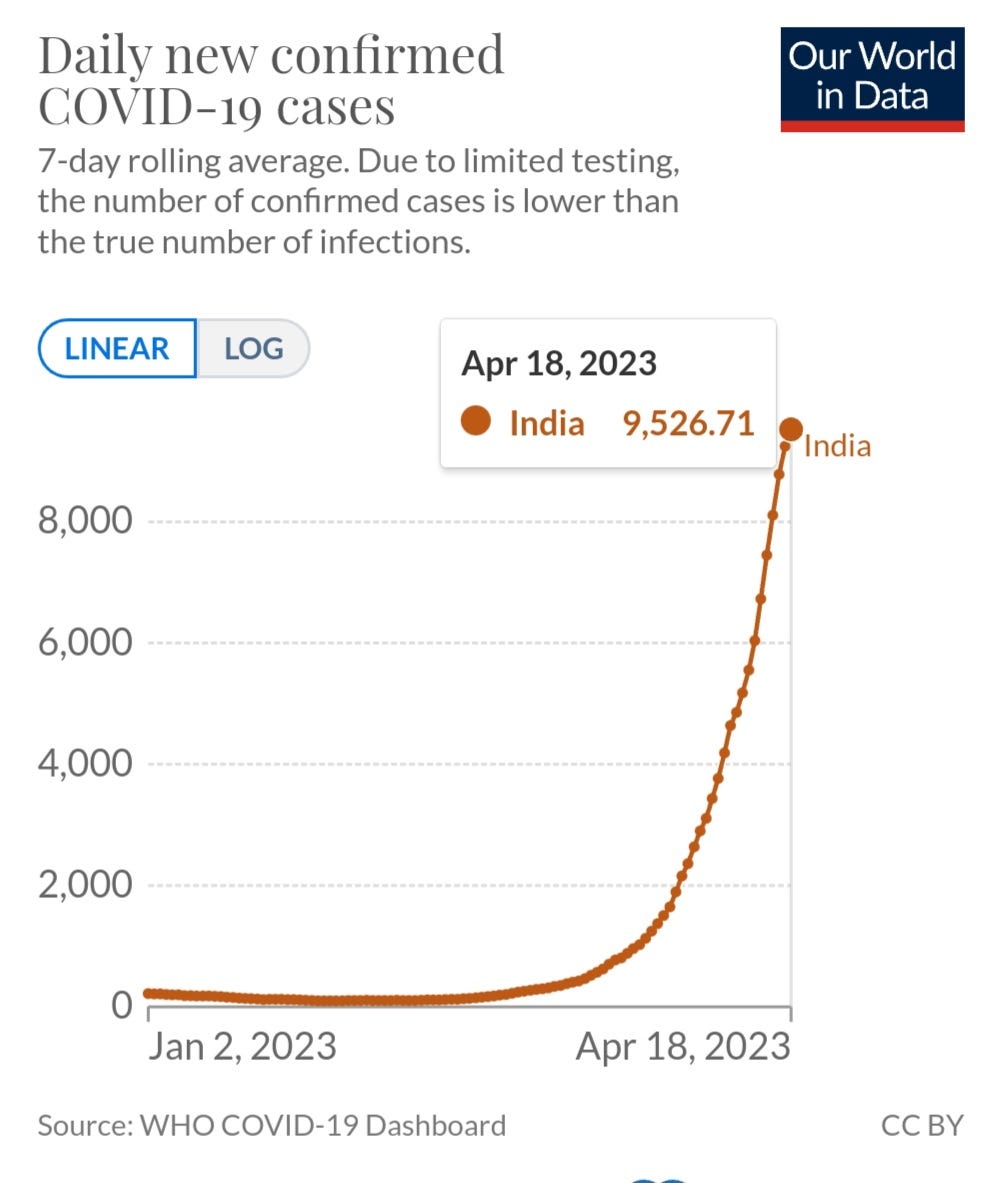
India Hits the Highest Level of New Cases in Eight Months
India records a 20% increase of new cases from the prior day and the most new cases in eight months. They added 12,591 new cases and 40 deaths. Our world in Data only shows through April 18th but we can see the trend. We know that they aren’t testing much, even in hospitals so the true numbers are much higher but the concern is that despite this the level of cases and deaths continue to grow at an exponential rate. This means that the current variants are evading the population level immunity that XBB.1.5 wasn’t able to break through.
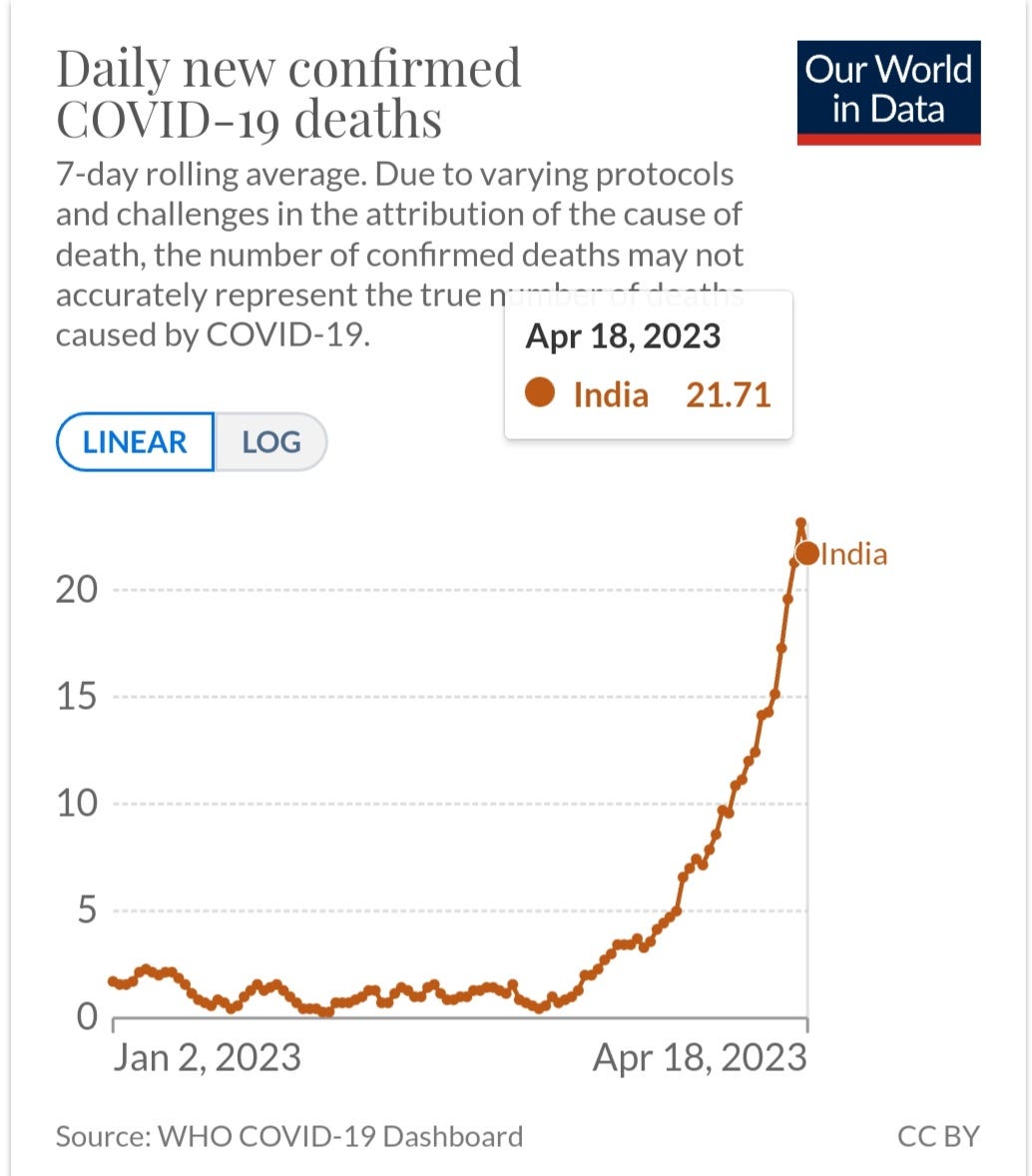
The same trend is occurring with new deaths (graph below). April 18th shows 21 deaths and on April 20th they are reporting 40 new deaths. The current variants are clearly taking a toll. The deaths and hospitalizations only show a small view. The much bigger impacts are likely going to be the secondary infections, like pneumonia, taking hold in the weeks and months ahead. The amount of people that will end up with persistent infections will likely increase, causing chronic conditions in millions more people, affecting the quality of life, the education of children, the healthcare costs will ruin many families futures, and ultimately shortening lifespans.
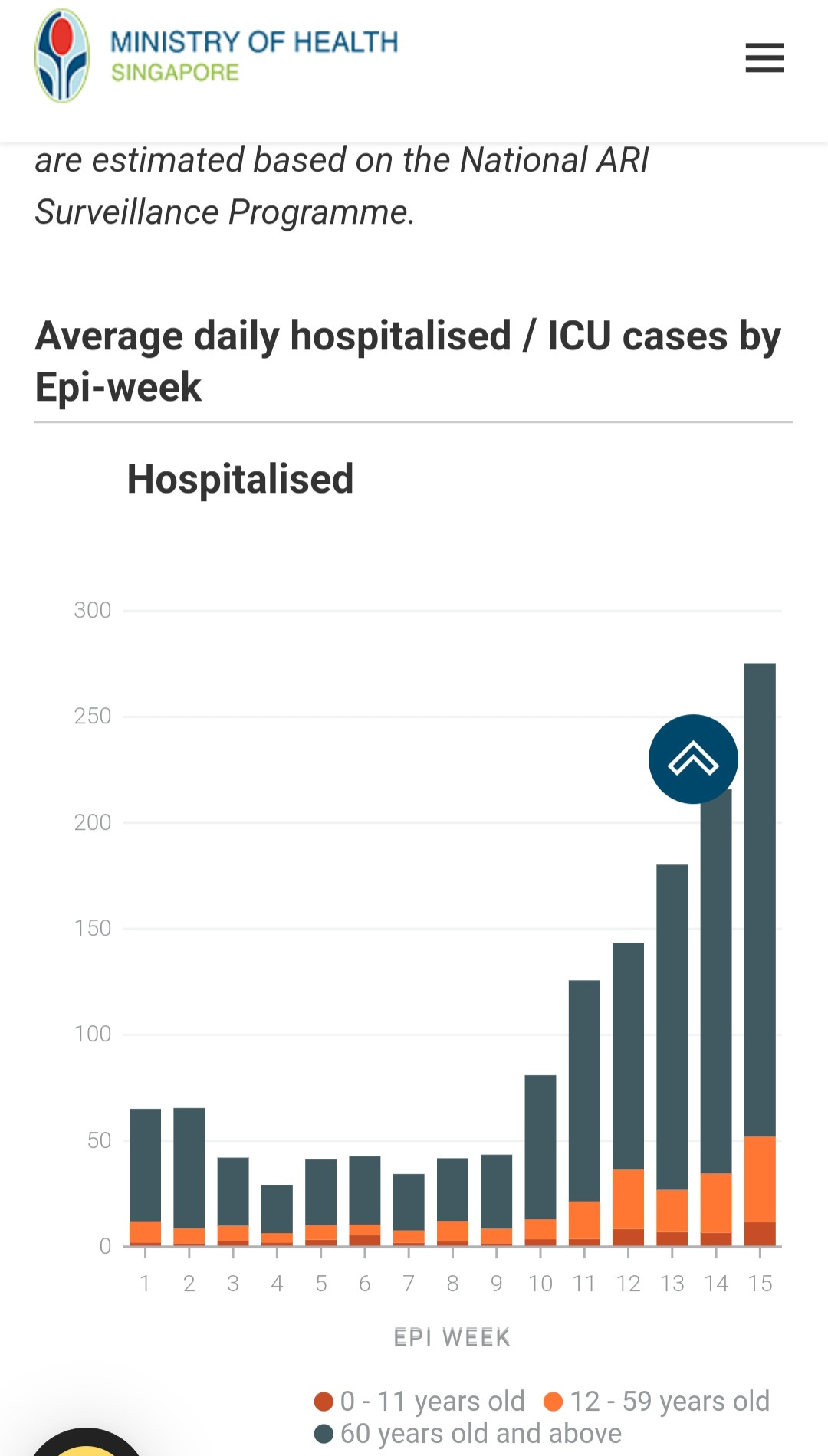
Singapore and India also have another sub-variant quickly rising to between 20% and 40% of cases. XBB.2.3 is up to 30% of sequenced cases in Singapore. Between the XBB.1.16 and its sub-variant, XBB.1.16.1 and the XBB.2.3 sub-variants, hospitalizations are increasing in Singapore, India, Indonesia and Vietnam. (Singapore shown below)
Hospitals Could Become Breeding Grounds for New Variants
XBB.1.16 and XBB.2.3 are developing new mutations in the body of the virus and the spike at an alarming rate. It is important to remember that removing masks in hospitals can increase the risk of immunocompromised patients becoming infected with multiple variants, which can lead to the creation of new, stronger variants that can evade treatments and our immune system. If universal mask use is not maintained in healthcare settings, hospitals can become a breeding ground for new variants and a dangerous environment for patients, causing many to avoid seeking necessary care. Therefore, removing masks is a failure to fulfill an important responsibility.
Wearing N-95 masks properly can significantly reduce exposure to airborne pathogens, including COVID-19, RSV, and the flu. Therefore, surgical masks should be replaced with N-95 masks/respirators to protect patients from airborne pathogens in hospitals.
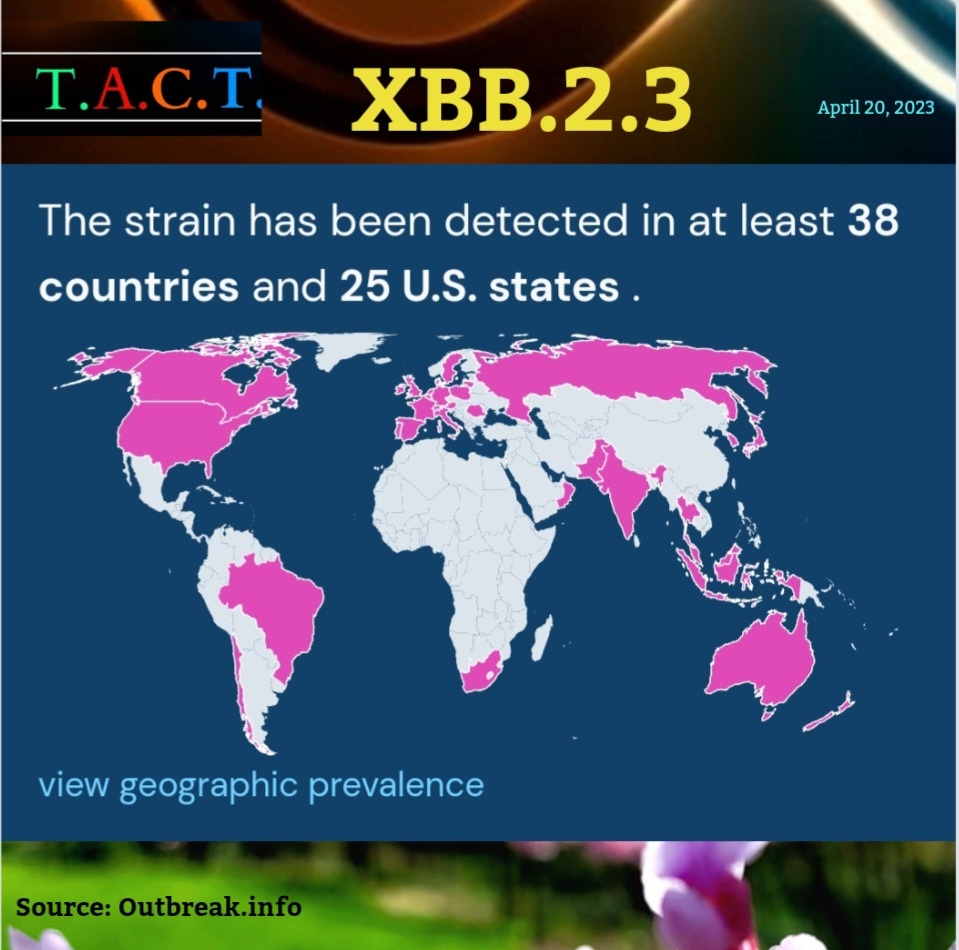
We are seeing that XBB.2.3 and its sub-variants are spreading at a rapid pace. This is a problem because the virus is changing in ways that make it harder for our immune system to fight it off. This means that even if you're healthy, you might not show any symptoms until you get a second infection or start having problems with your organs weeks or months after you catch the virus. This could increase your risk of having a stroke, heart attack, or getting an autoimmune disease.
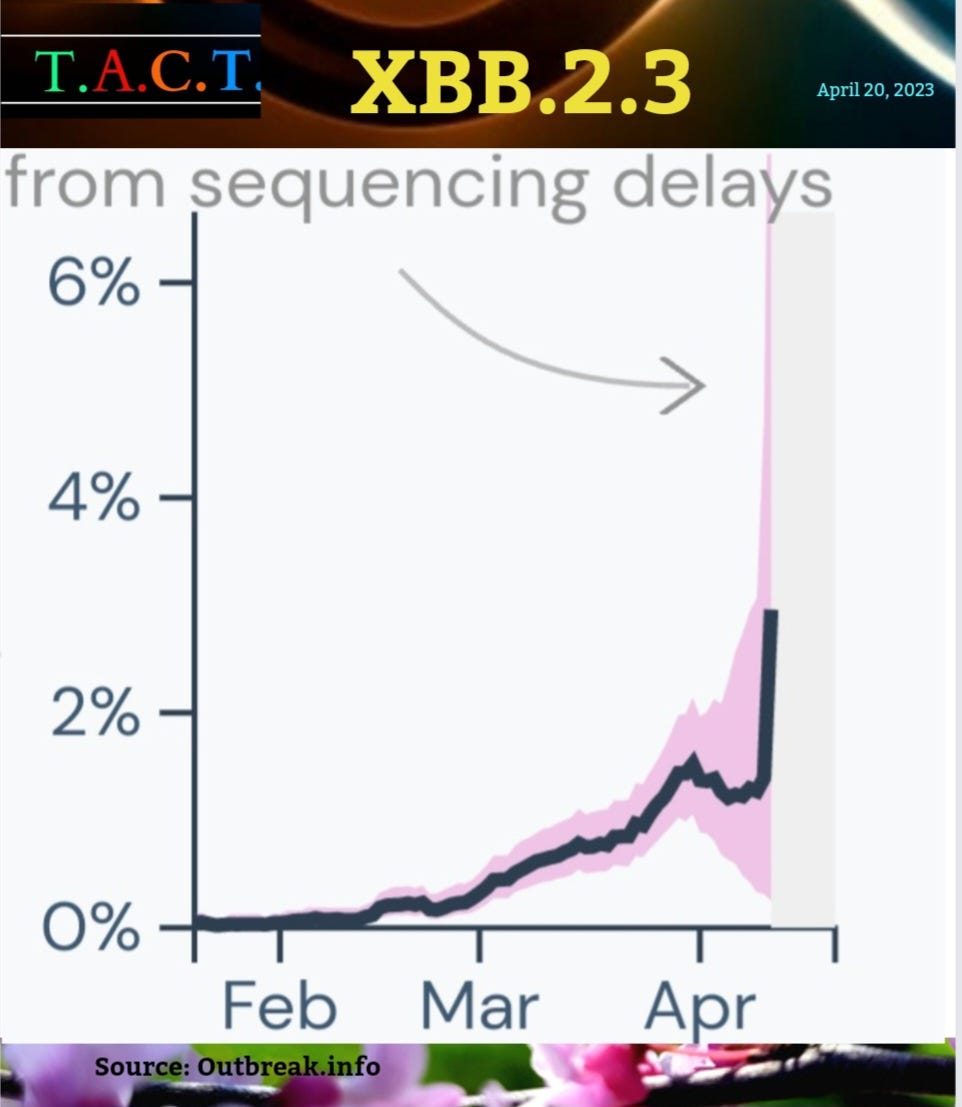
XBB.2.3 Prevalence in the U.S.
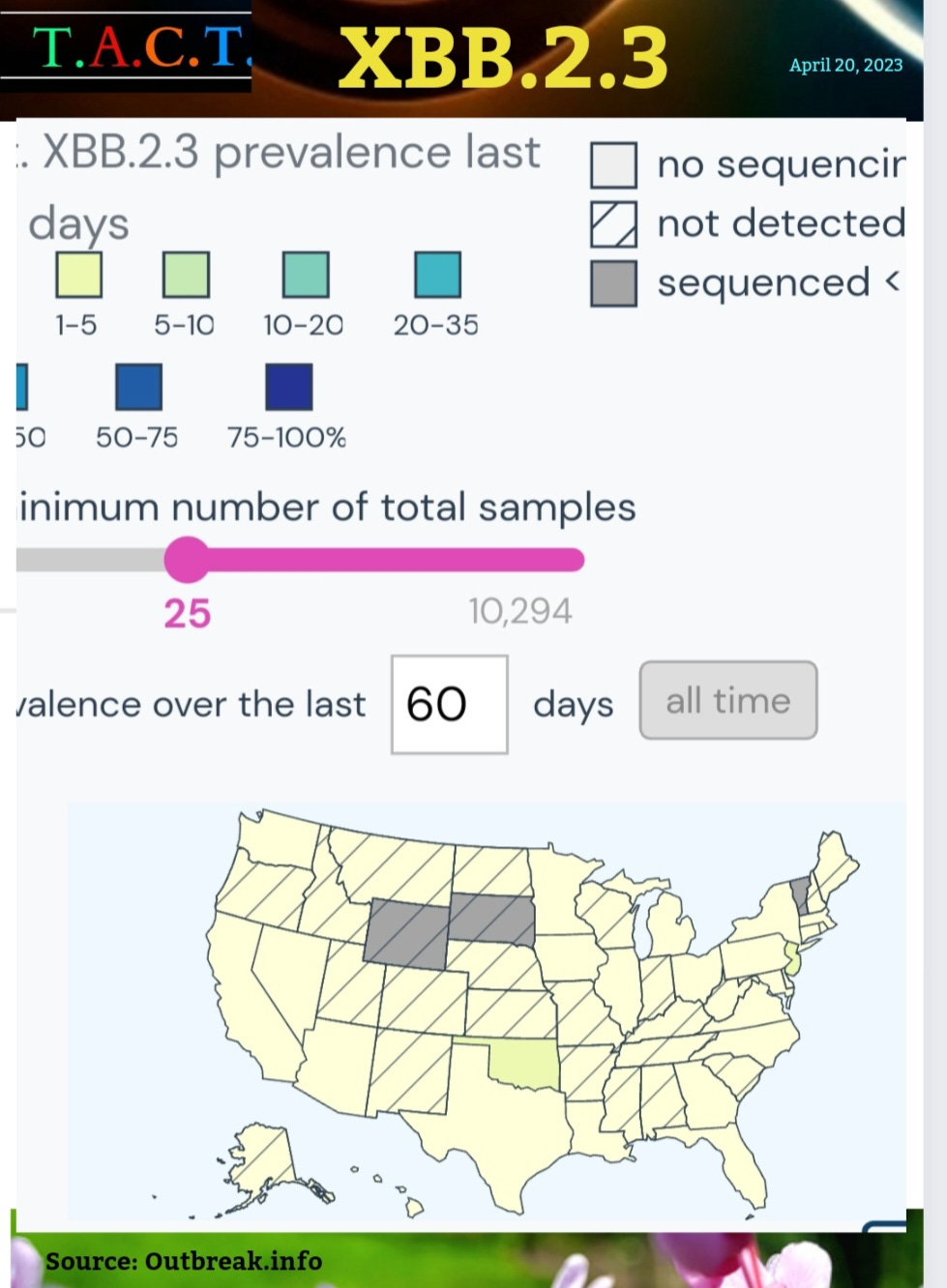
COVID has had an evolutionary advantage over us from the beginning. It can rapidly evolve around our immune system responses and treatments. The more treatments we use during widespread transmission, the stronger the virus becomes. Our evolutionary advantage is that we can build tools to significantly reduce transmission, but we are not investing in the necessary systems to give us that advantage.
If we take proactive steps to increase filtration and ventilation to maintain CO2 levels at 600 ppm with HEPA level filtration, we can be more at ease. Since that hasn't happened yet, this variant will likely spread quickly through schools and homes. Closing schools for summer break a few weeks early should not be ruled out. Schools should use the extra time to invest in systems that can significantly reduce transmission. This would be a significant step towards preventing the endless waves of illness and death, protecting children, parents, communities, and economies for years to come. It is the single most important thing we can do as a society to invest in our future. We must work Together Against COVID Transmission.
The media and public health officials would have us believe that COVID has become less dangerous and is no longer a major concern. The media coverage has nearly vanished. Independent sources that are not beholden to large donors, political parties, or any other group are more important than ever. Consider becoming a paid subscriber or donating a subscription to help support this work. Thank you for your support.
T.A.C.T. is a publication supported by its readers. Consider becoming a free or paid subscriber if you are not already a member of the T.A.C.T. community.
Please let us know what you are seeing or if you have any other insights or questions.

We now see how bankrupt doctors and hospitals are. The mask has literally been torn off their facade. They no longer care about the welfare of patients. The concept of Do No Harm is gone. Johns Hopkins Hospital will be ceasing universal masking effective 4/24/23. The only place masks will be required is " for patients on isolation precautions, for sterile procedures in the OR and other areas, and as part of standard precautions." There is no mention in the new mask protocols for masking in pediatric or adult oncology centers, or in transplant clinic areas, or rheumatology clinics.
They are literally throwing the immunocompromised to the dogs.
And where is the outcry from doctors and other health care workers. The concept of the Hippocratic Oath and Do No Harm is gone. We now see doctors and hospitals for what they are - people/institutions who don't care who they infect so long as they get their bottom line back in order.
The Twitter thread below by Yunlong Cao seems REALLY profound, although somewhat beyond my attenuated intellectual capacity. The 6th tweet down in the thread about immune imprinting and the dynamic evolution of the virus driven by the immunological history of the host is incredible. It's like the virus looks over each victim, analyzes the specific capabilities of that victim's immune system, then does a viral code 'required update' to bypass the victim's immune system. Perhaps this happens at the 'population level', such that different geographical regions might end up with their own specifically tailored variant selected especially for them.
Not sure I have this right. Look forward to your upcoming posts.
https://twitter.com/yunlong_cao/status/1649523529422082048