



Biden Tests Negative and Returns: Ignoring the Ongoing COVID Crisis
Biden Continues to Overlook COVID and Long COVID Realities

Biden has once again downplayed the significant risks of COVID, showing a lack of understanding and empathy for those suffering from Long COVID or those currently infected and unable to work or access the same treatment he is receiving. His disregard for the potential rebound after Paxlovid treatment, its limited efficacy against Long COVID, the threat of exposure to more evolved variants, and the possibility of becoming contagious again demonstrates a concerning lack of awareness.
President Biden is getting at least 10 days of Paxlovid, because Biden’s doctor, Dr. Kevin O’Connor, said he completed his 8th dose on the 21st and will continue treatment, which highlights how his access to treatment is not what the average person can get.
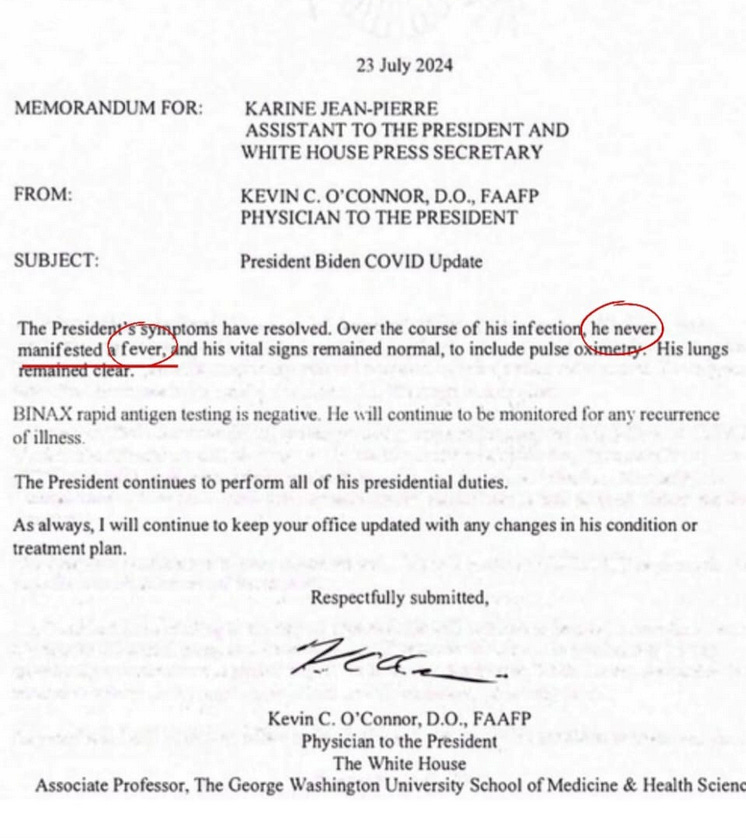
Biden's lack of a fever isn't noteworthy, because it's uncommon in COVID cases. Only around 15% of people have fevers. It's one of the least common symptoms.
As a reminder, the common symptoms (from the top/ most prevalent to the bottom/less prevalent) include:
Cough/ Dry Cough
Sore throat
Shortness of breath or difficulty breathing
Fatigue
Congestion or runny nose
Sneezing
Muscle or body aches
Headache
Diarrhea
Sinus pain
Fever or chills
Nausea or vomiting
New loss of taste or smell
Keep in mind that on average only 15% of people were found to have fevers. A fever is an unreliable indicator for determining if it's COVID or for ending isolation. Rapid tests are the best way to know when not contagious anymore.
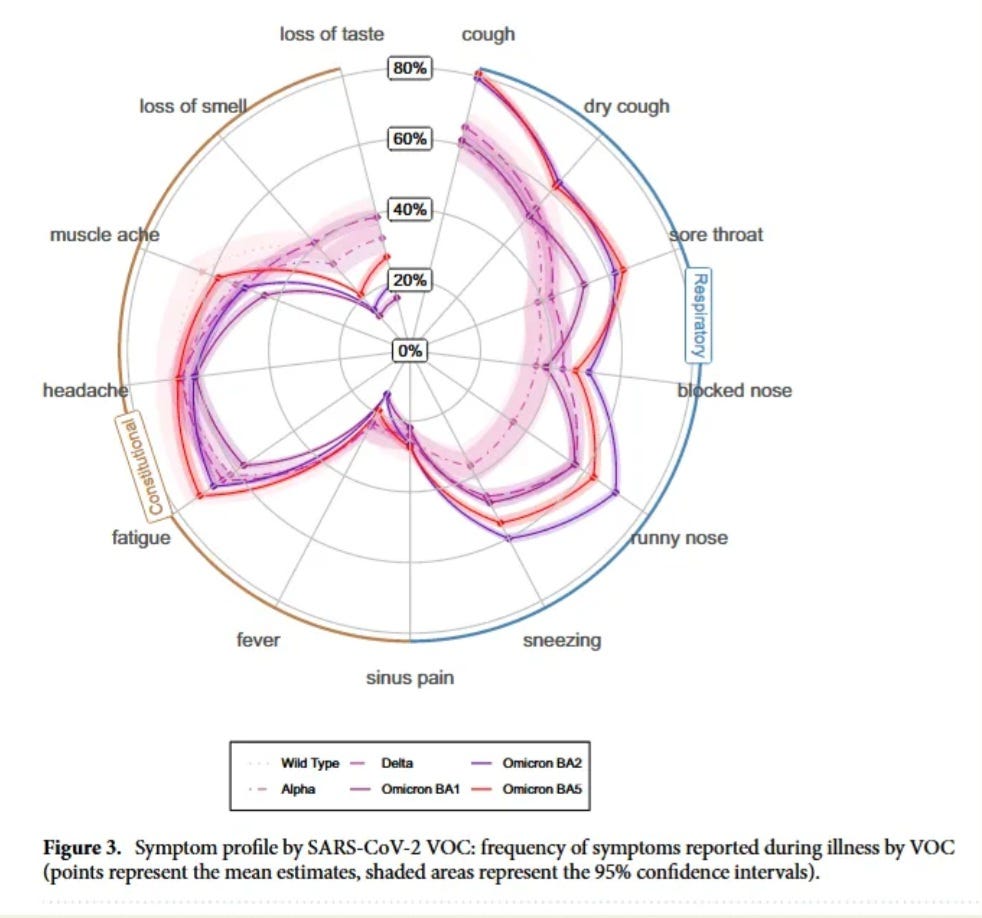
The diagram below, from a large study published in Nature, shows the percentage of people with each symptom across multiple variants. Loss of taste or smell are the only symptoms less common than a fever.
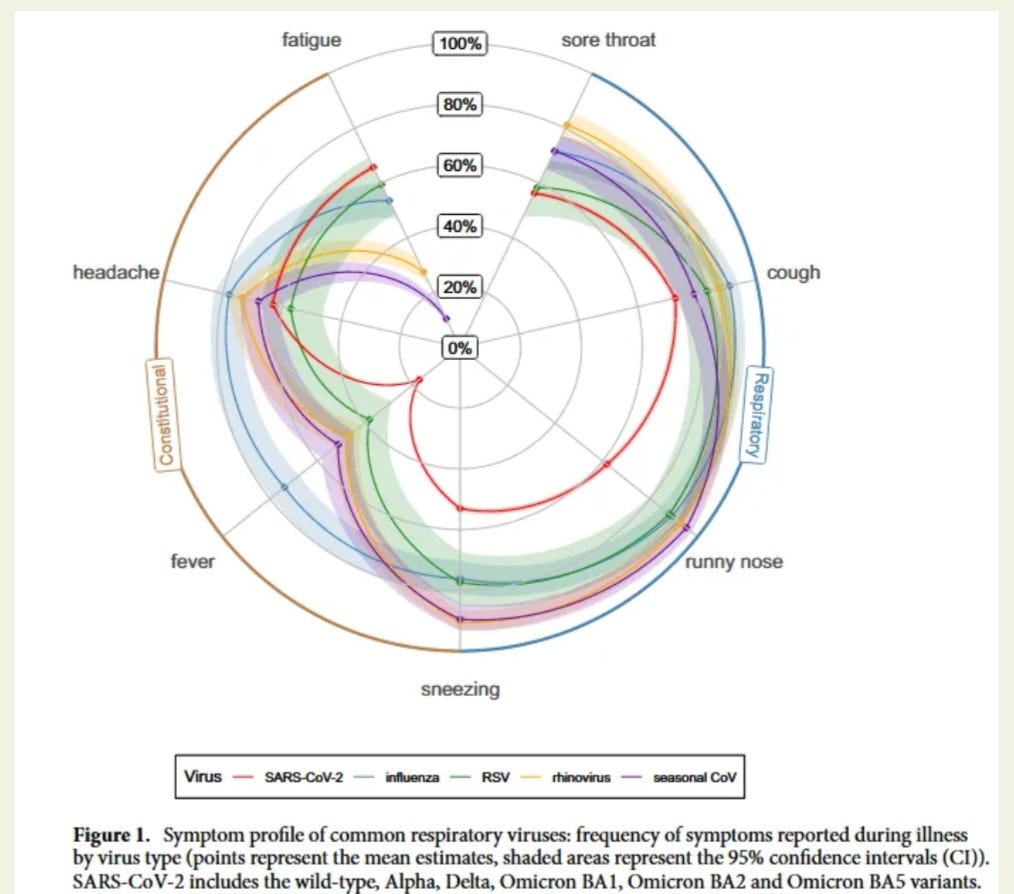
If we look below, at a broader view of symptoms across multiple viruses, having a fever is still one of the least likely symptoms.
Symptom severity varies widely, from asymptomatic cases to those requiring hospitalization. Even asymptomatic individuals can spread the virus and potentially develop long-term health issues.
Testing remains crucial for accurate diagnosis and appropriate management of COVID-19. Speaking of testing, it’s important to note that the FDA’s web page that is updating us on tests that may become ineffective due to new mutations, “SARS-CoV-2 Viral Mutations: Impact on COVID-19 Tests”, hasn’t been updated since September 28, 2023! Is anyone verifying the efficacy of existing tests against the latest variants?
The letter highlights how the 24-hour fever-free guideline for return to work/school is flawed and was never backed by larger studies or cumulative data. Many other symptoms would be a better measure, but we know that many people feel better after 4 or 5 days, which is still too soon to go out into public because most people remain contagious for at least 8 to 10 days, regardless of having symptoms.
This is from TACT’s March 13, 2024 post on how long people remain contagious and the negative repercussions of reducing the isolation period below 5 days to only 24 hours after a fever.
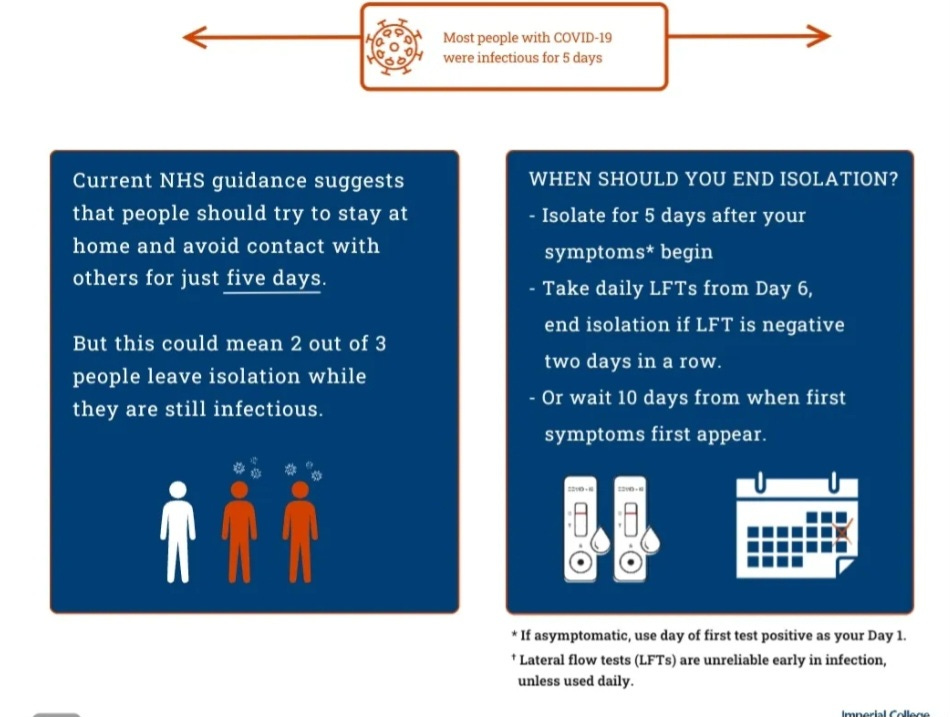
A real-world study led by the Imperial College London and published in The Lancet Respiratory Medicine journal found that in people who develop symptoms, the majority are not infectious before symptoms appear, but two-thirds of cases remain infectious five days after symptom onset. This was during earlier variants, but again confirming most people were still infectious on day 5.
These findings, along with numerous other studies, consistently indicate that individuals typically remain infectious for a minimum of 7 to 8 days, with a considerable number remaining infectious for 10 to 20 days.
A significantly more effective approach, rooted in scientific evidence, is outlined in the graphic above from the Imperial College of London. It suggests a protocol of isolating for 5 days followed by testing on day 6 to assess continued infectiousness. Repeat testing on day 7 helps confirm the results. If negative, it's likely that the individual is no longer infectious and can safely end isolation. However, if the test is positive, continued isolation is necessary.
Following isolation, it's recommended to use a quality N-95 or similar mask for an additional 2 to 3 days while interacting with family members or being in public spaces to further reduce the risk of transmission.
It's particularly crucial to highlight this approach in light of the recent CDC update on isolation guidance. The shift from the previously recommended 5-day isolation period to just 24 hours after a fever, without testing, lacks scientific basis and isn’t grounded in logic. It should be retracted immediately. Failure to do so could have detrimental effects on all levels of society.
We are seeing this in real-time as COVID surges to new heights this July, going into August, surpassing previous years across many areas of the U.S., Europe, and other countries around the world. All of this transmission escalates viral evolution making it even less likely that spike protein-targeted vaccines will offer benefits against the circulating variants by the time they are approved and released.
If you are a visual learner, the radial diagram of the variants being sequenced over time shows very clearly what is happening. As mitigation measures were removed through 2021 and 2022, the pace of new variants started gaining momentum. By 2023 the XBB variants were dominating and variations continued to grow. As we moved into 2024 through to July 2024, we have seen an explosion in the evolution. Where do you think this will go in 2025?

The constantly high level of circulation of new variants with surges multiple times a year leaves more people susceptible to persistent infections with one or more variants. According to Biden’s doctor, Biden was infected with the KP.2.3 variant. According to the CDC’s updated variant proportions, KP.2.3 makes up around 12.8% of cases. Biden is risking exposure to a more evolved COVID variant while he is still recovering which could put him into a much worse situation.

KP.3.1.1 has much higher ACE-2 binding and greater immune evasion than the KP.2 variants. A co-infection with a KP.3.1.1 variant while still fighting off the current variant could be very dangerous for him.
A human host harboring multiple COVID-19 variants poses significant health risks and contributes to the virus's ongoing evolution. With millions potentially persistently infected with one or more variants, the opportunity for the virus to adapt to treatments increases. A variant may remain within a host for years, and if that person is later infected with another variant, it can lead to the emergence of a more evolved, hybrid variant that could escape and spread widely. This trajectory is unsustainable. We must change our behaviors and invest in technology to effectively control transmission.
Given Paxlovid rebound risks, even after 10 or 20 days of treatment, Biden should not resume work, especially when putting himself face to face with many people. He should be resting and strengthening his immune system. Considering the odds of rebound and lack of benefit in preventing Long COVID based on the latest studies shown below, he may become positive again, increasing the odds of Long COVID and risks exposing more people to infection.
From TACT’s post on May 4, 2024 “Metformin vs. Paxlovid: The Urgent Need for Metformin's Approval in COVID-19 Treatment”
The CDC tells us effective treatments are widely available, but are they? Monoclonal antibodies are no longer effective, and the cost of Paxlovid is out of reach for many people. Paxlovid often isn’t prescribed by doctors because Paxlovid may not be safe to take for specific individuals for a wide variety of reasons. In comparison, metformin has a long history of having a very good safety profile.
A study from January 4, 2024, found that between a group that was given a placebo and a group that was given Paxlovid, “about 16% of those treated with Paxlovid had long COVID symptoms compared to 14% of those who were not treated with the medication."(6)
Somewhat surprisingly, it found that “among those at high risk for severe COVID-19 we estimated average treatment effects of 0.032 using propensity matching and 0.012 using nearest neighbor matching, both consistent with no benefit of treatment." (5)
As far as symptom rebound with Paxlovid, "26.1% reported rebound symptoms or test positivity."(6)
On January 12, 2024, a study was published on the efficacy of Paxlovid in COVID patients with Metabolic-associated Fatty Liver Disease (MAFLD)
The researchers investigated the impact of MAFLD on disease severity, outcomes, and the efficacy of Paxlovid (nirmatrelvir/ritonavir). This is important because, MAFLD, affects around a quarter of the world's population.
They concluded that “no significant distinctions were observed in hospitalization duration, oxygen saturation, or severity based on MAFLD status.” (7)
"Never manifested a fever" distracts from more crucial concerns like how will this impact his cognitive function and overall health. It's downplaying the risks associated with every COVID infection.
From TACT’s post on January 14, 2023, “COVID Brain Infection” “Appearances can be Deceiving. What we know and what we don't know.”
There is no doubt that COVID can infect the brain, cause structural changes, and last for months or longer, even if the first symptoms are mild. This doesn't appear to impact everyone but appearances can be deceiving.
We know quite a bit about the mechanisms and pathways COVID uses to impact the brain but we don't know what percentage of people are being impacted to lesser degrees. Is there a lower level of damage that people are rationalizing as being caused by other things? How will this affect people later in life? We do know that it already affects millions of people to some degree. We know that 100's of thousands are unable to work because of this disease affecting their minds. We also know that early onset dementia after COVID is occurring.
As a society, we should work to protect everyone, particularly given the massive numbers of people impacted by this brain infecting virus. The worst part is that each time COVID adds mutations, it gets better at suppressing the immune system and infecting organs.
COVID has defeated all the available monoclonal antibody treatments and is outpacing targeted vaccines. It has strengthened its grip onto ACE-2 receptors making it more infectious. Remember we have these receptors in our eyes, ears, nose, throat, lungs and all throughout the body. It enhanced its ability to evade antibodies and attack cells of the immune system. It has also become more capable of infecting organs, including the brain.
The consequences of ignoring this will surely impact everyone, directly or indirectly, in some way. After reviewing the mechanisms of how the brain is infected and impacted we will show some strategies, based on the science, that when used together can significantly improve your odds of avoiding infections with COVID and, if infected, help limit the odds of infecting the brain. With any luck, prevent it from seriously impacting the brain.
1. This "study demonstrates structural and functional alterations in the brain tissue of COVID-19 patients which correlate with neuropsychiatric and neurological dysfunctions."
"SARS-CoV-2 could access the CNS through the neural-mucosal interface in the olfactory mucosa"(1)
In other words, COVID can infect the brain through the deeper section of the nasal passages. (see below on how to reduce the odds of infection through the olfactory mucosa.)
2. "We show that astrocytes are the main locus of infection - and possibly replication - of SARS-CoV-2 in the brains of COVID-19 patients, as evidenced by the detection of the viral genome, the SARS-CoV-2 spike protein" (2)
Astrocytes are essential for the formation and maintenance of the BBB (Blood Brain Barrier) by providing secreted factors that lead to the adequate association between the cells of the BBB and the formation of strong tight junctions.
"The blood–brain barrier (BBB) is a tightly regulated interface in the Central Nervous System (CNS) that regulates the exchange of molecules in and out of the brain, thus maintaining the CNS homeostasis. It is mainly composed of endothelial cells (ECs), pericytes, and astrocytes that create a neurovascular unit (NVU) with the adjacent neurons.”
“Under neurological disorders, such as chronic cerebral ischemia, brain trauma, epilepsy, Alzheimer's disease, and Parkinson’s disease, a disruption of the BBB takes place, involving a loss in the permeability of the barrier and phenotypical changes in both the Endothelial Cells and Astrocytes." (2a)
Let's review what this says. Astrocytes and endothelial cells are essential for maintaining the Blood Brain Barrier (BBB), which must remain strong to prevent brain diseases, like Alzheimer's and Parkinson's disease.
COVID infects astrocytes and endothelial cells, which may disrupt this cohesive framework. COVID also infects neurons. People are having brain fog, and early onset dementia after having COVID. Does anyone see the seriousness of a virus that can infect these cells?
3. "A neuroimaging study reveals significant brain changes in areas associated with language comprehension, cognition, and circadian rhythm control six months after COVID-19 infection."
Take note that this says, "six months."
If that weren't bad enough, we already know that COVID can survive in the brain and other organs for longer than 6 months.
"The researchers also found a significant difference in the right ventral diencephalon region of the brain stem. "This region is associated with many crucial bodily functions, including coordinating with the endocrine system to release hormones, relaying sensory and motor signals to the cerebral cortex, and regulating circadian rhythms (the sleep-wake cycle)."
“This study points to serious long-term complications that may be caused by the coronavirus, even months after recovery from the infection,” Mishra said. “The present findings are from the small temporal window. However, the longitudinal time points across a couple of years will elucidate if there exists any permanent change.”
"The researchers are conducting a longitudinal study on the same patient cohort to determine whether these brain abnormalities persist over a longer time frame." (3)
4. "We were able to detect the virus in the oesophagus, large intestine, kidney, placenta, lung, and brain." (4)
This is what they tested with the less immune evasive variants.
The risk will increase with variants like XBB.1.5 and whatever comes after it.
5. "Alzheimer's-like signaling in brains of COVID-19 patients"
"The neuropathological pathways causing tau hyperphosphorylation typically associated with Alzheimer’s Disease were also shown to be activated in COVID-19 patients. RyR2 in COVID-19 brains demonstrated a “leaky” phenotype, which can promote cognitive and behavioral defects." (5)
6. "SARS-CoV-2 infection and persistence throughout the human body and brain"
"Our data prove that SARS-CoV-2 causes systemic infection and can persist in the body for months." (6)
Strategies to Avoid COVID and a COVID Brain Infection. Scroll to the bottom of the post “COVID Brain Infection”. Click HERE.
President Biden had the chance to address critical COVID issues, especially now that he's not burdened with a reelection campaign. Unfortunately, that opportunity is being missed, which is why TACT is here to highlight these concerns.
Support TACT's mission by becoming a paid subscriber. For just $8 a month, or $80 a year, you can significantly contribute to this effort. Your support is greatly appreciated!
If a subscription isn't possible, please share our posts, refer friends, and help spread this important information. Growing our community is essential for the change we seek. We must work Together Against COVID Transmission.
Please share any insights, questions, or stories in the comments.

Seems like the White House physician tried VERY hard to get Biden to generate a negative test. BinaxNow? Really?
Note that the White House only discloses that Binax was Negative. The results from any OTHER viral testing are not reported.
A rectal swab evaluated by PCR might produce an entirely different result.
Nasopharyngeal swabs can go negative BEFORE intestinal samples.
"Faecal viral metagenome of three patients continued to display active viral infection signature (higher 3’ vs 5’ end coverage) up to 6 days after clearance of SARS-CoV-2 from respiratory samples."
https://gut.bmj.com/content/70/2/276
Excellent points regarding Biden's criminal minimizing of the Covid pandemic and his most recent infection raises more questions such as, when did #GenocideJoe 's covid infection really begin? Is it possible that he was infected as early as before the debate when he said he had a cold? As I have already written in a comment to a different article here, my son who PCR tested positive first told me that he had only cold symptoms for about 10 days before he developed a slight fever, acute fatigue and back pain. After 2 days, he went and tested positive. Ergo, is it possible that there is a new variant that presents more slowly than previous variants did? Regardless, it is a fact that Biden was campaigning unmasked indoors for days before it was reported he had tested covid positive and even then the video of him after his positive test revealed that when he got out of the car to get on Air Force 1 in Las Vegas he was unmasked and then after he departed Air Force 1 in Dover, Delaware he was still unmasked exposing all the Secret Service personnel driving in the cars with him. Finally, when he exited his car to get back on Air Force One for returning to D.C. this past Monday, he had a surgical mask in his hand that he must have been wearing that last time in the car on the way to Dover Air Force base. See here: https://youtube.com/shorts/lFR1fvh85iY?si=vGKswTq7k9z97KIA