



The Next Wave: XBB.1.9.1, XBC and XBB.1.5 sub-lineages. Why are the advantages gained so concerning?
Evolution is starting to occur in the body of the virus instead of the spike, which suggests it is working around the strong T-cell response the majority of people have acquired.

XBB.1.9.1: Child of Recombinant BJ.1, BM.1.1.1. This variant started out in Southeast Asia and is spreading at an exponential pace in Australia, the U.K., the U.S., Canada, and other parts of Europe. At least 4 cases were sequenced in Ontario, Canada, up through January 21st, so it is likely much more widespread already.
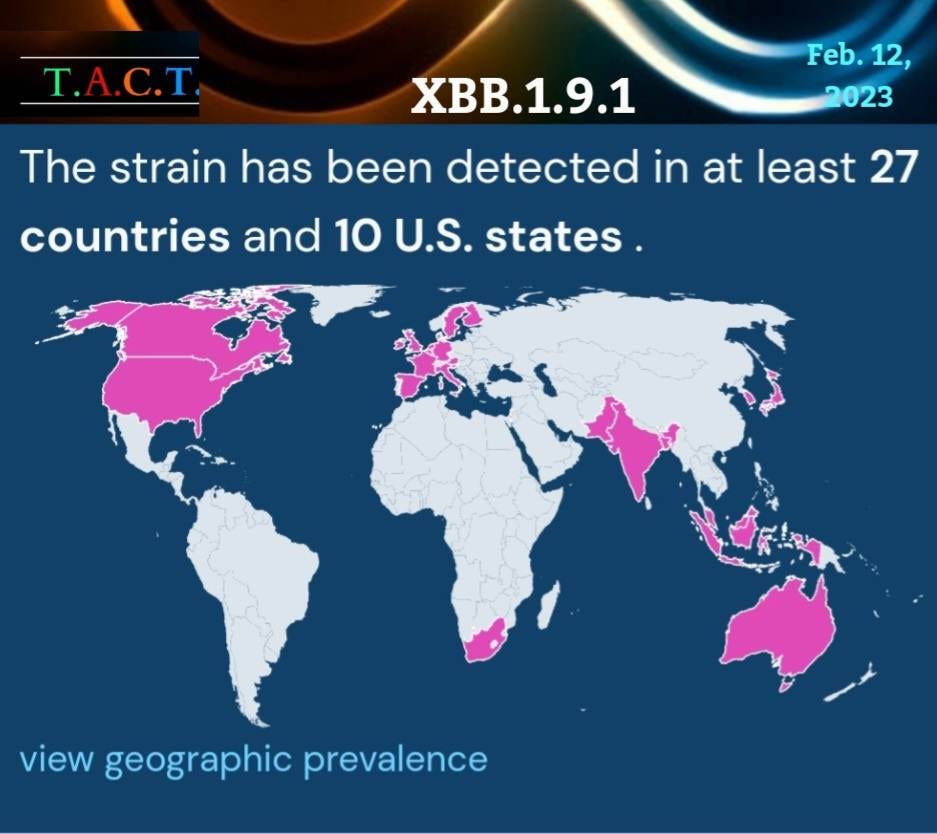
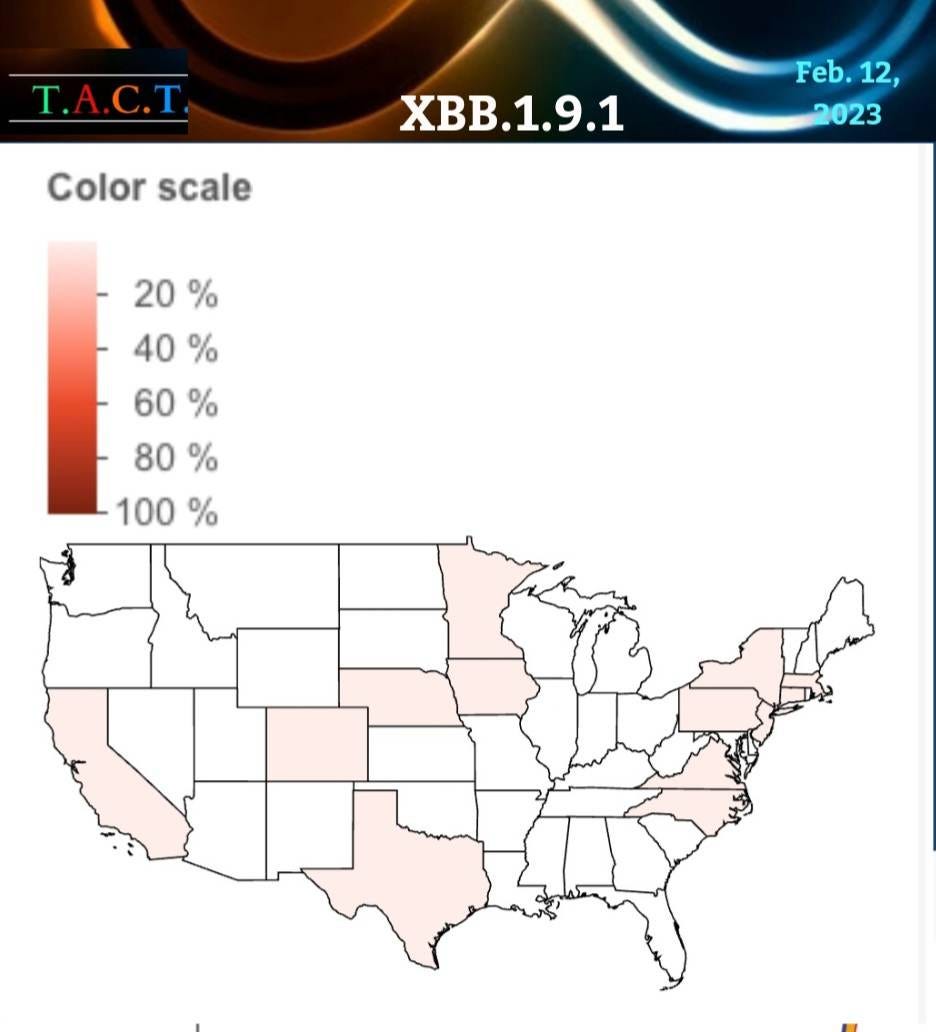
According to even more up-to-date data, the XBB.1.9.1 variant is in 14 states, but is likely much more widespread than this due to the delays in time between someone testing positive, the case getting sequenced, and then reporting that data.
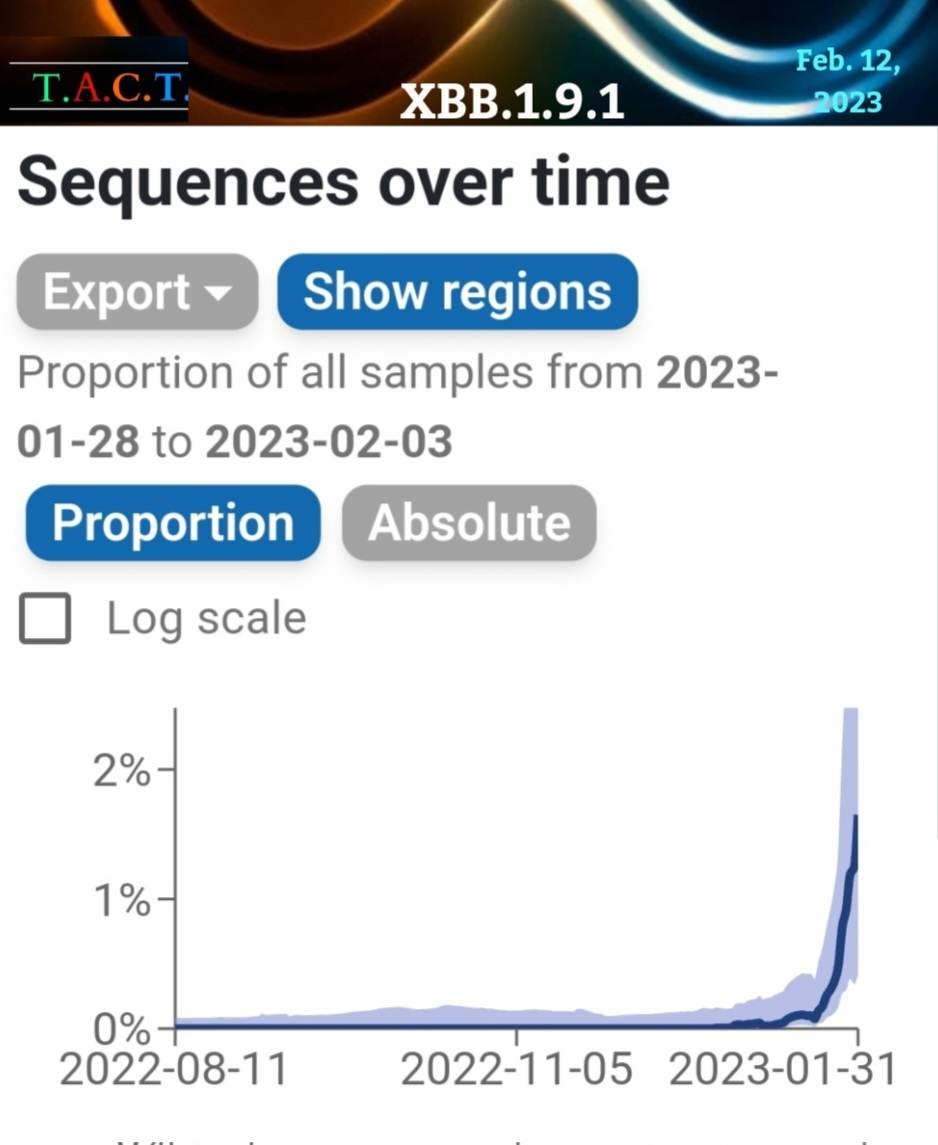
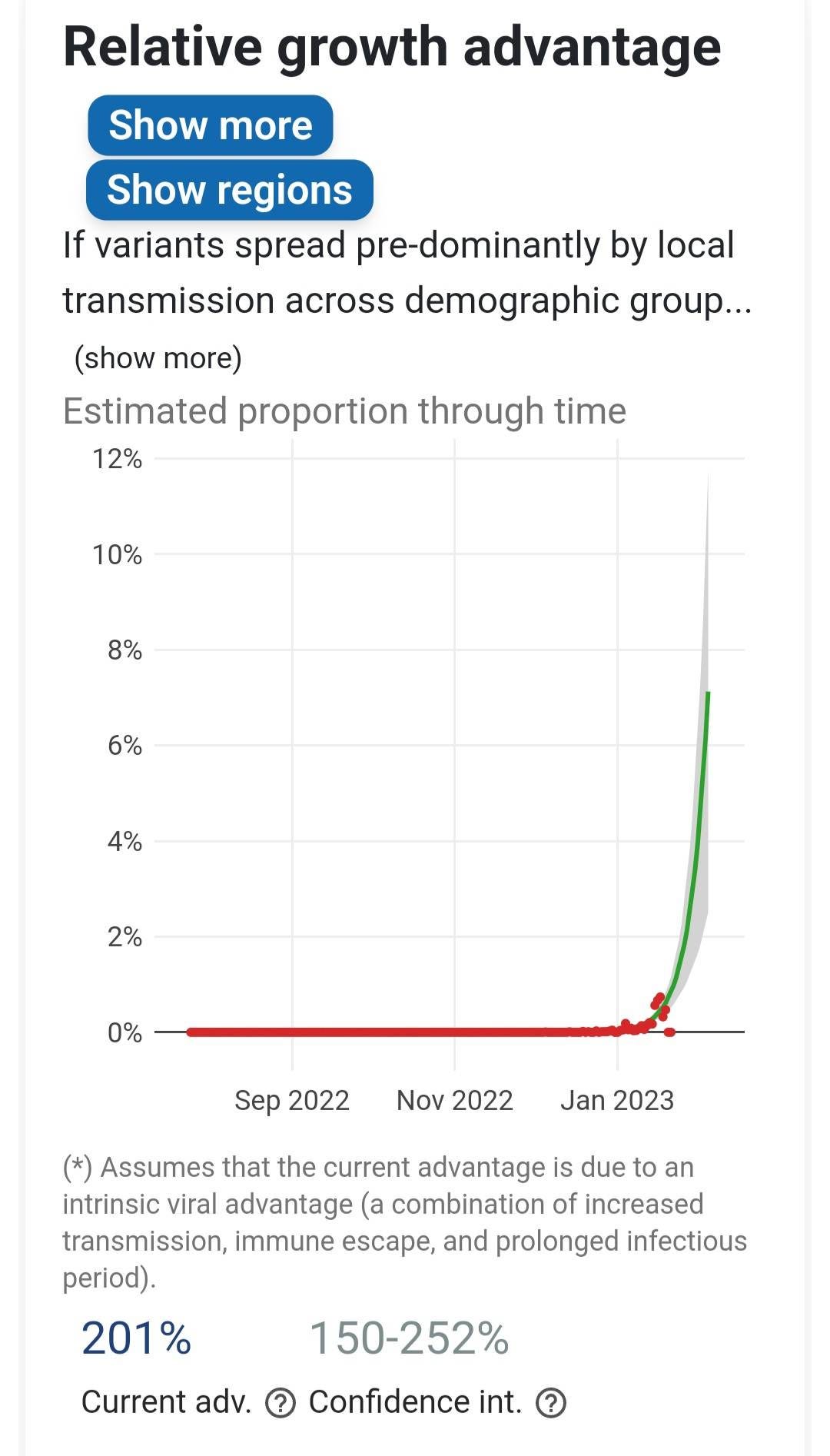
To give an idea of how much it has spread, we can see in the graph below, that it already makes up between 5% and 10% of sequenced cases in Singapore, the U.K., and Austria.
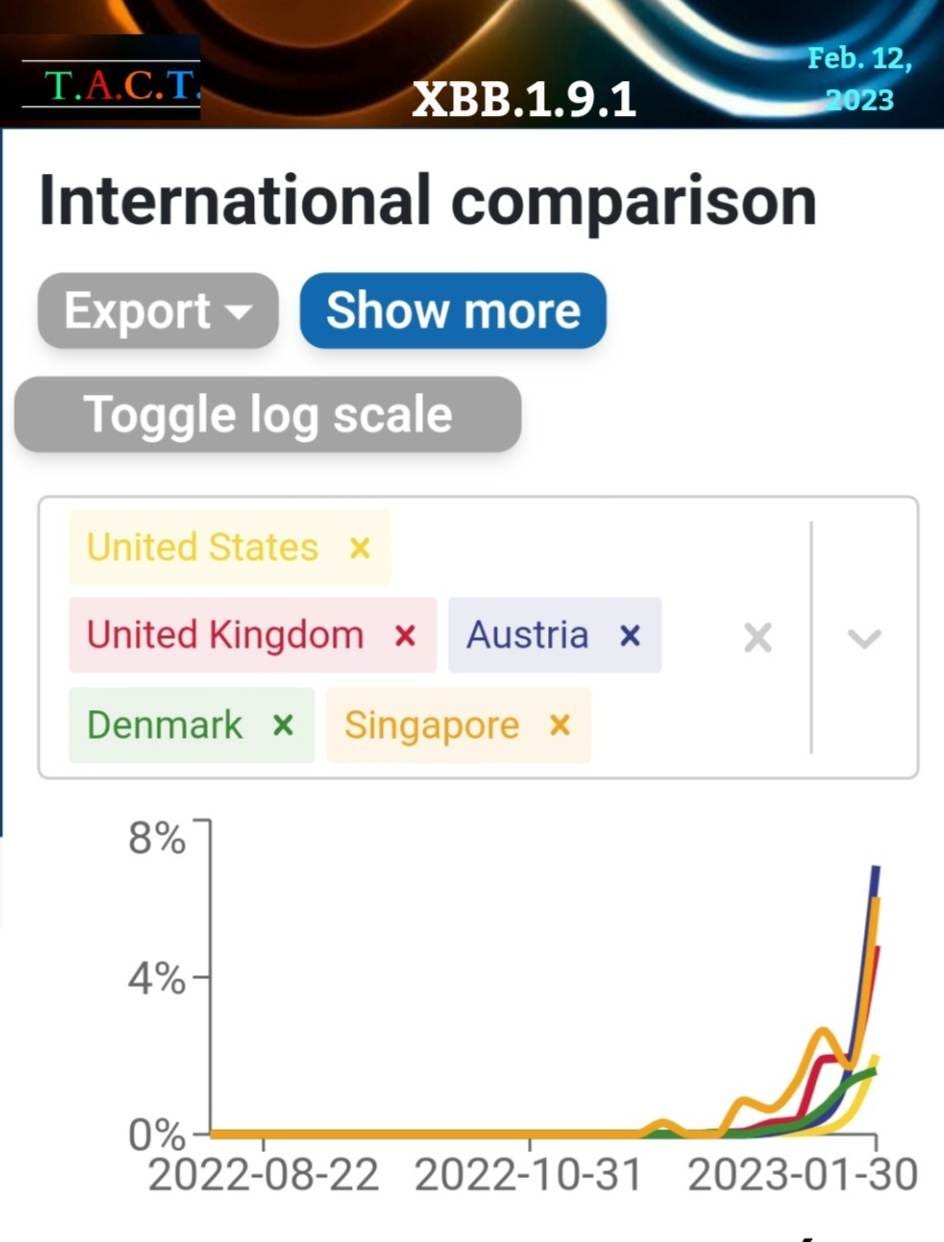
Singapore had a huge XBB wave a few months ago, so clearly this new XBB variant is infecting people again. This is spreading as Singapore removes the mask mandate for public transportation today. Luckily, the majority of people in Singapore are still wearing their masks on public transport despite the requirement being removed.


The rate of its growth in the real data matches the estimates of its growth advantage. The question that we must ask is, "What is giving this variant an advantage over XBB.1.5?”
XBB.1.5 is the most common variant in Ontario, Canada, and the U.S., with a large number of cases in many other countries. However, the next wave of variants will soon take its place at the top. XBB.1.5 is the most antibody evasive variant to date, defeating all the available monoclonal antibody treatments, and evading antibodies from recent infections and the BA.5 bivalent boosters. That means everyone is susceptible to infection and long term persistence in organs and other viral reservoirs, like men’s testicles. Fertility rates were declining before COVID. We may have a very real problem on our hands in the years ahead.
The XBB.1.5 variant is the most immune suppressive variant to date, and like variants before it, it is causing vascular dysfunction, which can lead to heart attacks & strokes. Because heart attacks and strokes often occur after the initial infection, people may not test positive when they are brought in as patients, therefore aren’t recorded as deaths from COVID. All the available science and data tell us that the excess deaths in young and middle age adults are caused by COVID.

If XBB.1.5 is already so good at evading antibodies and suppressing the immune response, then how could the next wave of variants outcompete XBB.1.5? The answer is probably not what anyone wants to hear, but it is important to understand where this might be headed next.
In the history of modern virology, SARS-CoV-2 has made more new variants and lineages than any other virus. Even though the SARS-CoV-2 vaccines reduce severe illness and death, they don't give enough immunity to keep vaccinated people from getting sick again, allowing the virus to replicate and mutate. Because of this, we have the strange situation where a virus replicates in a host while the immune system forces the virus to change in ways that make it resistant to both vaccine-induced immunity and infection-induced immunity. The answer to what it will do next is to avoid or attack the next layer of the human immune system more effectively.
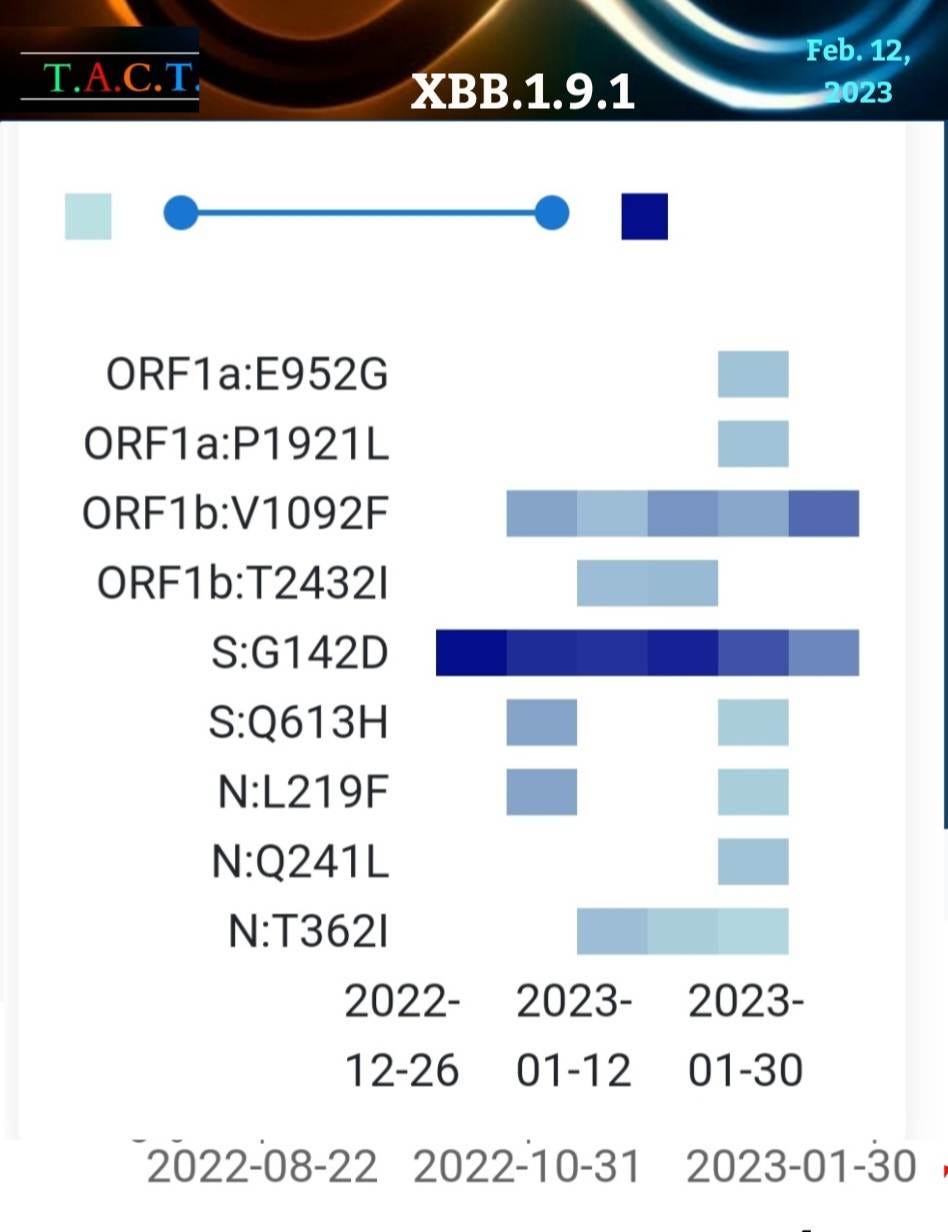
The N:T362I, N:Q241L, and N:L219F mutations jump out because it is yet more mutations in the N-protein, not the S-protein. These mutations impact T-cells, our last line of defense. “The SAR-CoV-2 N-protein plays pivotal roles in inflammation, cell death, innate antiviral immunity, and adapted antiviral immunity.” (1)

How could changes in the N protein give COVID an advantage?
The XBB variants crushed the antibody response, so what is the next best way for COVID to gain an advantage? If it were to gain a competitive advantage over XBB.1.5 by a mutation in the N-protein, then the most likely answer is to beat the next most common immune response. That is the T-cell response. Selective pressure tends to dictate COVID’s evolution.
“The adaptive cellular immune responses rely on both CD4+ T cells to secrete cytokines for the functional support of CD8+ T cells and B cells, and on CD8+ T cells to eliminate the virus by killing infected cells.” (2)
We have a study that discusses mutations of N361-N369, and as shown in the picture above, the XBB.1.9.1 mutation, N:T362I, may give this variant a unique advantage over XBB.1.5. “These results, particularly the different reactivity of NT362I and NT362K, implied that the charge of the amino acid side chain, at least, might influence the binding affinity of N361-369 to HLA∗A11:01*. We also found that the N361-369 homologous peptide from MERS-CoV (NMERS), which exhibited 3 amino acids in difference to N361-369, bound to HLA∗A11:01 weakly" "Interestingly, the TCR 4-T cells were mainly activated by N:T362I or N:F363L"(2)
If the N:T362I mutation activates CD4 T-cells, then that could increase viral replication while interrupting the job of the CD4 T cells in helping the CD8 T cells. At least one study has shown this is already happening. "Once inside T helper cells, SARS-CoV-2 assembles viral factories, impairs cell function, and may cause cell death.” “SARS-CoV-2 infected T helper cells express higher amounts of IL-10, which is associated with viral persistence and disease severity. Thus, CD4-mediated SARS-CoV-2 infection of T helper cells may explain the poor adaptive immune response of many COVID-19 patients." (3)
If the mutation prevents cytokines from being released, the immune response could be less effective. If it causes more cytokines to be released, there could be more inflammation and problems with blood vessels, leading to vascular dysfunction. Any changes that weaken or alter the T-cell responses could have serious implications. We don’t have data on what the other mutations in the N protein may do, but we do know that evolution is about survival, and the next best advantage is to keep breaking down our immune response.
The evolution of COVID continues in a very dangerous direction. We know that this virus has the capacity to become more dangerous. The more widespread the transmission, the faster the evolution. COVID is evolving at a faster pace than ever before. We have the tools to slow it down, but we aren’t using them. Instead, the governments of the world have decided to get rid of the tools we've been using to track and monitor this virus. This will hide it from all but the most dedicated COVID trackers.
The media and public health sources would like us to believe that COVID has become less dangerous and is not a significant concern. The media reports have dwindled to nearly zero. It is more important than ever to have independent sources that are not beholden to large donors, political parties, or any other group. Sign up as a paid subscriber today or consider donating a subscription. Thank you for your support.