



COVID Update: June 26, 2023-Variant Report
Mutation in ORF10 and the potential impact of this new variant.


United States
The CDC has changed its reporting of variants from once every week to once every two weeks so this is just one more area the brakes have been put on the information flowing out of the CDC. The President promised the tools to allow us to make decisions to protect ourselves based on individual risks but we have watched those promises fade away. The people at greatest risk have less ability than ever to assess the risk.
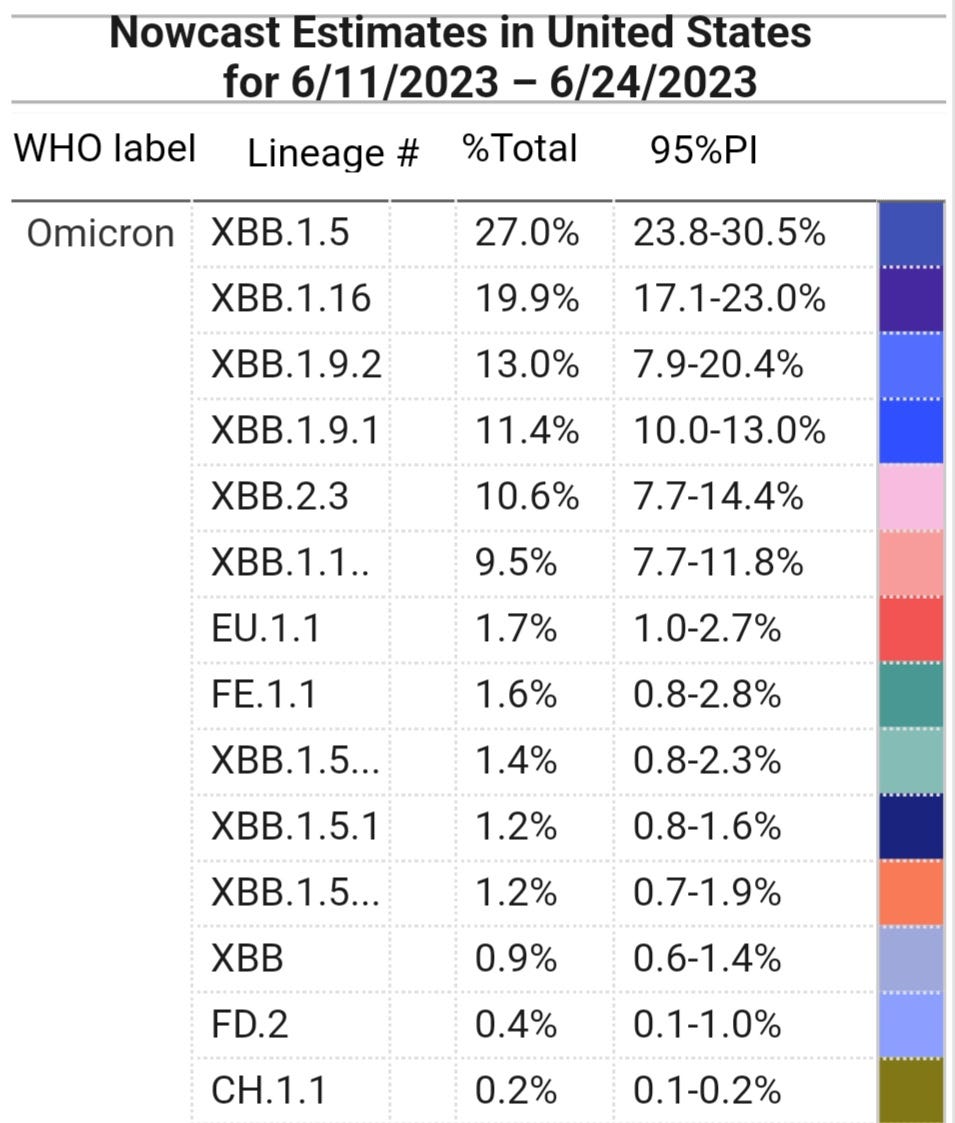
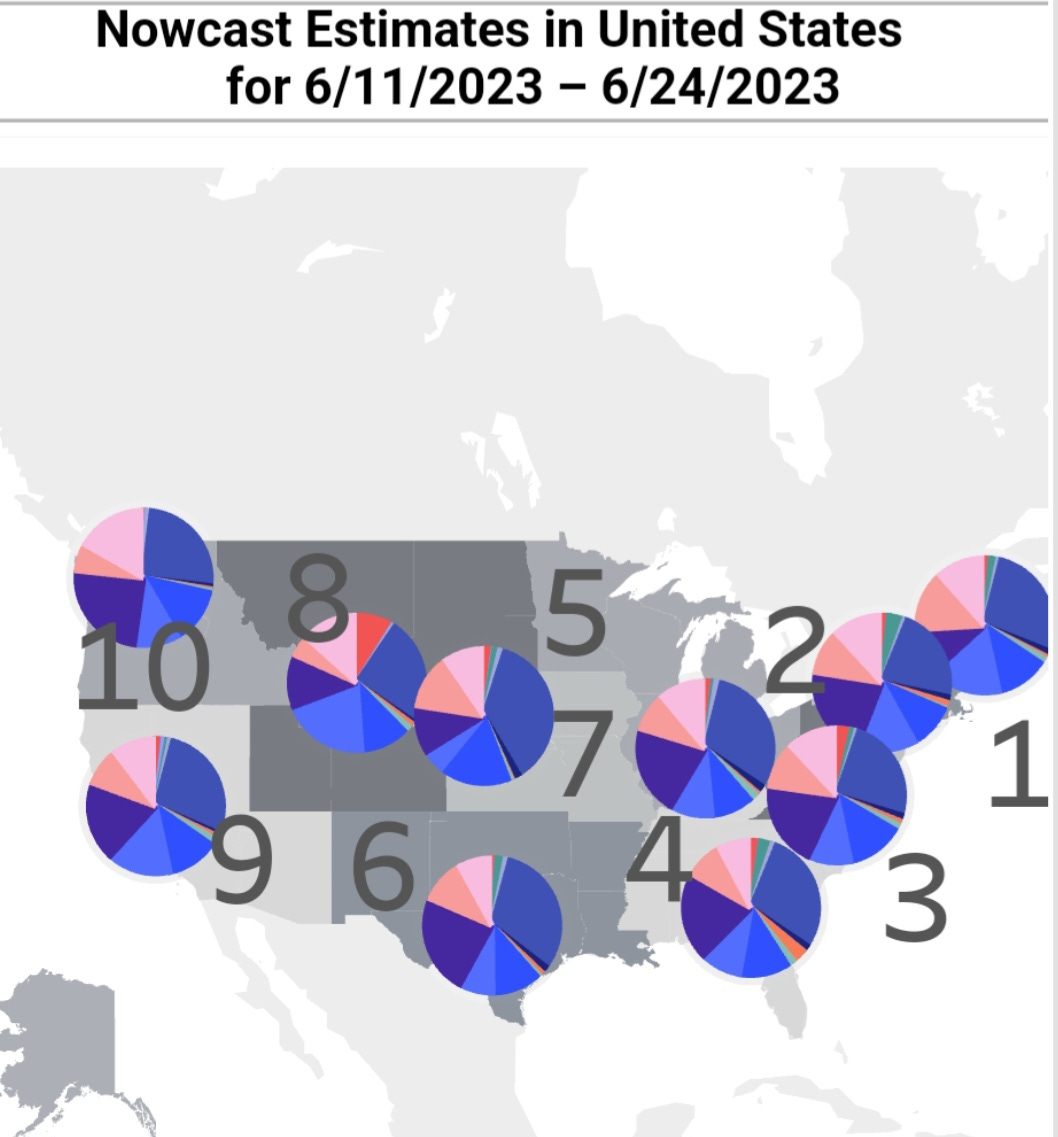
We can see from the graphs below that XBB.1.5 continues to decline while XBB.1.16, XBB.2.3, XBB.1.9.2, XBB.1.9.1, FE.1.1, and EU.1.1 are all gaining ground. All of these variants are the most immune evasive and suppressive variants we have seen yet. We can see that they are all grabbing a significant share of the pie. As the variants become better adapted at evading antibodies and T-cells or infecting T-cells, the immune response has been significantly diminished. People will have less symptoms while the virus makes itself at home. Persistent infections are likely to keep increasing, leading to autoimmune disorders, chronic health issues, earlier deterioration of the quality of life and ultimately shorter lifespans.
Every infection that bypasses antibodies, infects the cells of the immune system, the thymus, tonsils, and almost every other organ including the brain, is increasing the risk of persistent infections and shortening our lives. With more people than ever having mild symptoms or no symptoms, the risk of an inadvertent infection from someone close to you has increased. People that are testing are finding that the tests are often producing false negative results due to the tests themselves no longer detecting the variants, taking the tests to early, and/or only swabbing the outer edge of the nasal passage when swabbing the throat and saliva along with the nose has produced much more reliable results. An article from Jan 6, 2022, “'Swab your throat first and then your nose': 4 disease experts offer new guidance on COVID-19 rapid tests”.
Published March 2023, the study says, "Throat-swab and saliva viral loads began to rise as many as 7 days earlier than nasal-swab viral loads in most individuals, leading to very low clinical sensitivity of nasal swabs during the first days of infection."
In another study, "Overall, saliva is a reliable specimen for the detection of viral RNA, antigens, and antibodies. However, a standardized procedure for saliva sampling and processing is needed, especially for the detection of viral RNA."
Why are doctors still swabbing only the nose? The tests apparently aren’t coming with the longer swabs anymore. Only long enough for the shallow swabbing of each nostril. When do people go to the doctors? During the first few days of an infection. At every step of the way, the CDC, family or primary care doctors and/or pediatricians are failing to acknowledge and explain the risks and failing to diagnose COVID, while continuing to aid in its transmission and thus the evolution of the virus.
CDC Variant Proportions
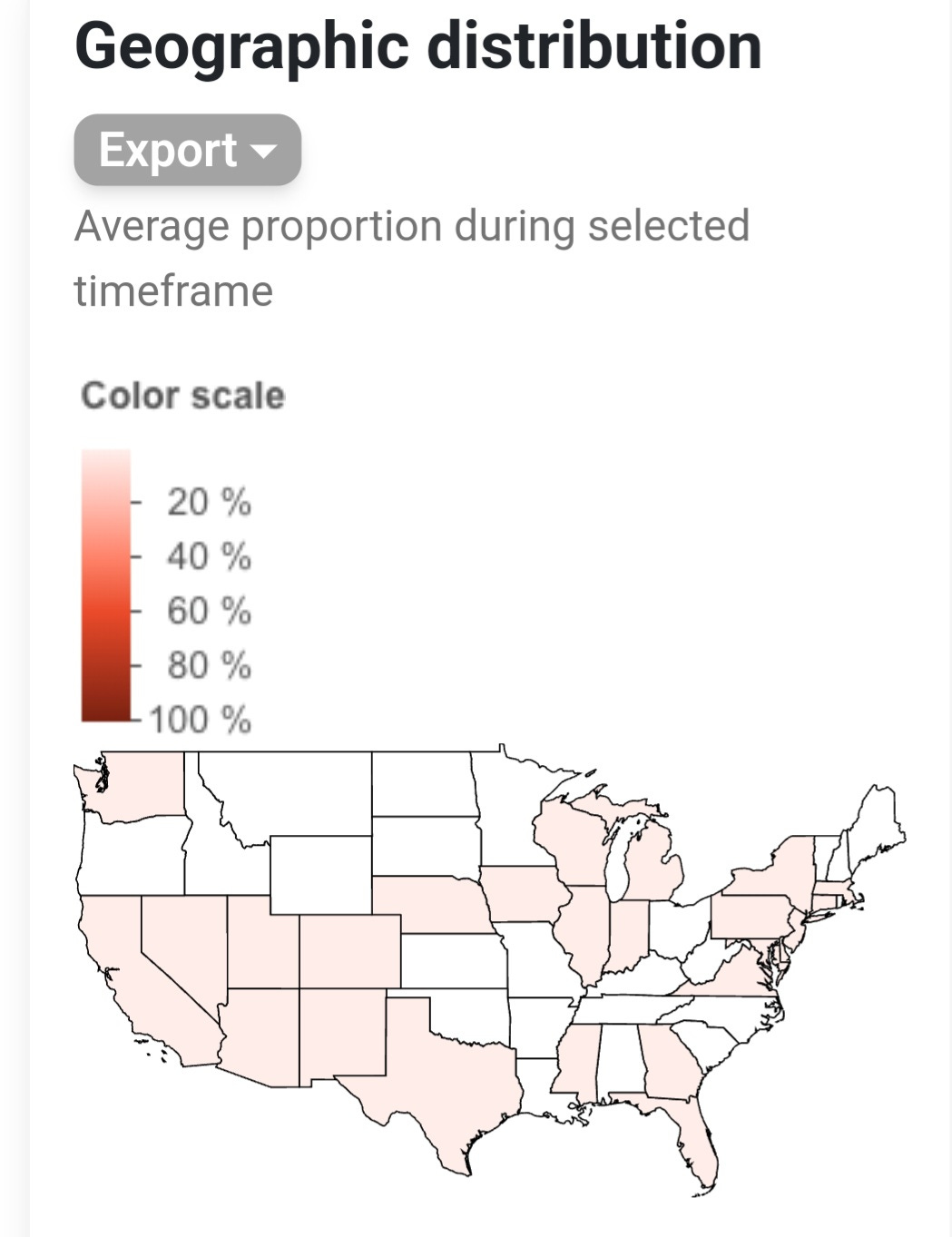
EU.1.1 (XBB.1.5.26.1.1) is now on the CDC’s radar currently most prevalent in Utah. EU.1.1 has two new mutations in the spike protein. S:I410V and S:P521S but only has a 1% advantage over XBB.1.16 (Arcturus). EU.1.1.1 is likely being placed under EU.1.1 on the CDC chart because this has an estimated 15% to 20% advantage over Arcturus. This is concerning but not as concerning as what we will discuss in more detail further down in this post. A variant that has a mutation in ORF10 with a 200% plus growth advantage over Arcturus. We will look at several studies showing how ORF10 helps evade the innate immune system and aids in replication.
If you aren’t a paid subscriber, please help support this work by becoming a paid subscriber but you can also sign up as a free subscriber. As a free subscriber you will get an email when this becomes available to everyone in a few days.
The chart below is from the CDC. It shows the variants they are most concerned about at the moment because they are most prevalent in the U.S.
EU.1.1, below, has been sequenced in 30 countries and 25 U.S. states. EU.1.1.1 has been sequenced in 21 countries and 6 states.
FY.3.1 (estimated >200% Growth Advantage over Arcturus (XBB.1.16)

FY.3.1 variant has an estimated 217% (9.76%- 425.68%) growth advantage over Arcturus (XBB.1.16). It’s most prevalent mutations are ORF1a:A2554V, ORF1b:Y1466H, S:H146Q, S:H146K', S:R683W, S:D950H, and S:I210T. As we can see from the graph below, it is increasing the most in China while only spotted a few times in other countries. Until something else emerges, this is the variant with the greatest potential to wreak havoc on the world. As shown below, it is taking off in China, but has been sequenced in 11 countries so far. We can expect this to spread at a fairly fast pace based on all the available data.
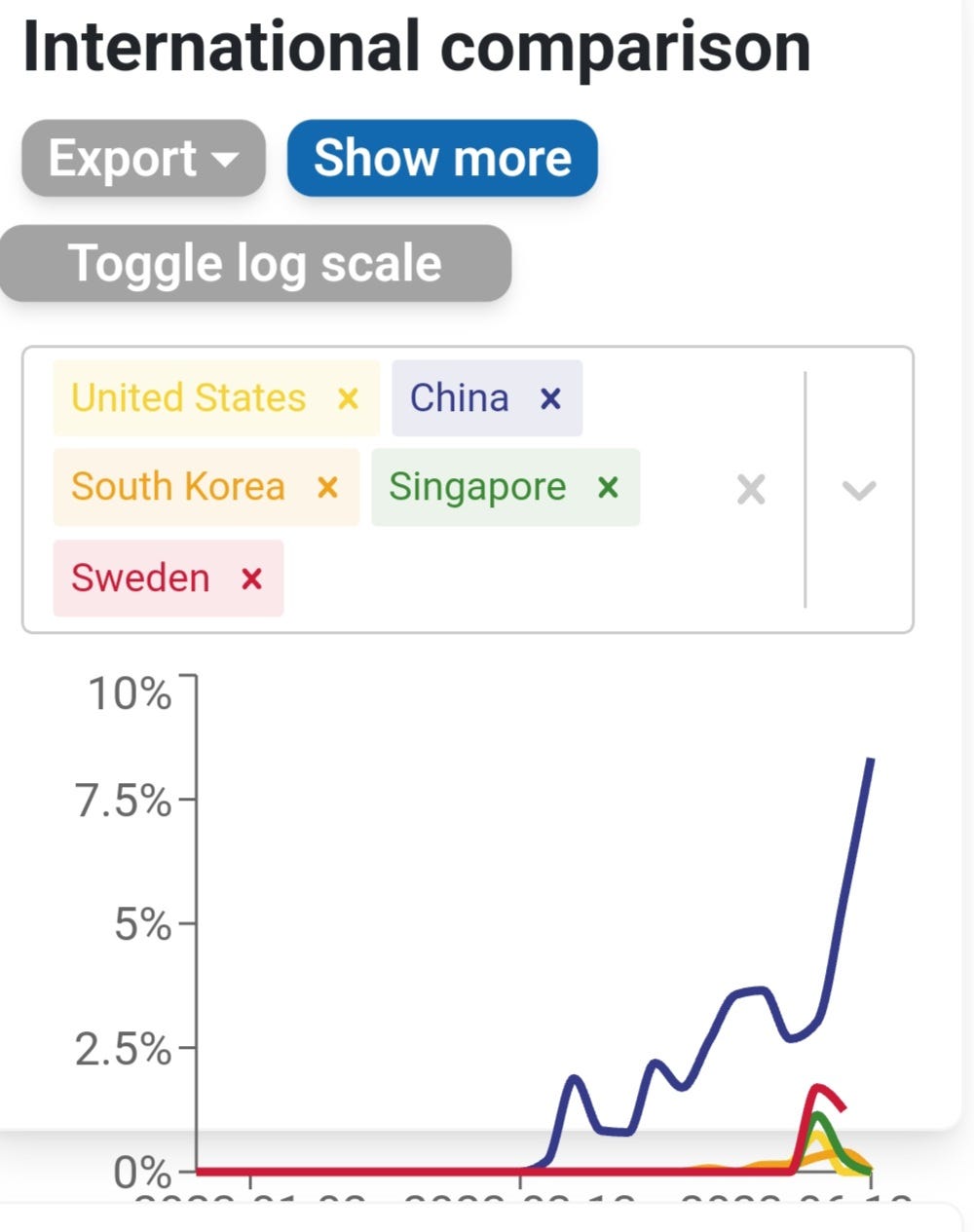
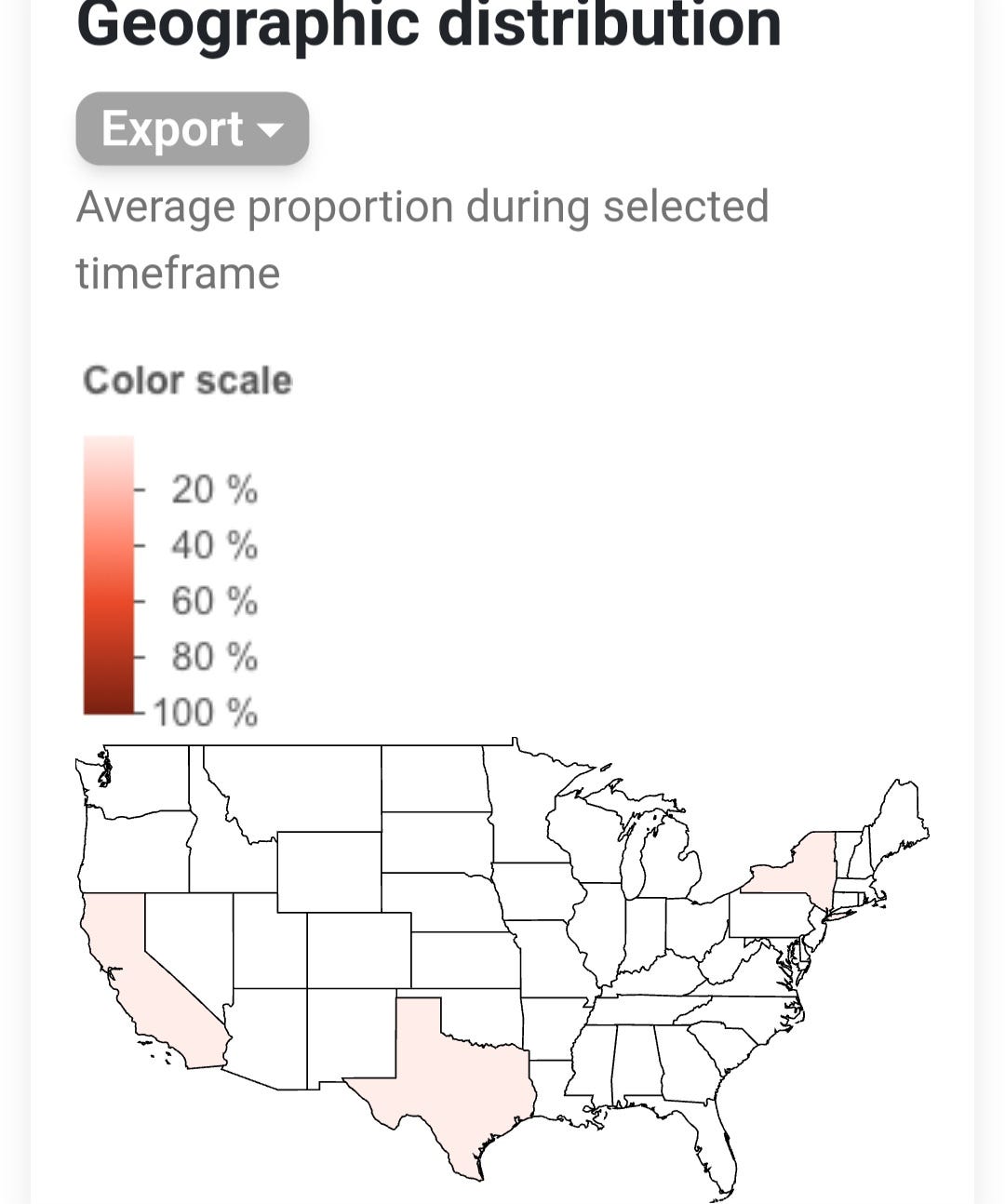
Besides the countries listed above, it has also been sequenced in Israel, Laos, Austria, Norway and France. The graph shows the drop back down in countries outside of China because it was only sequenced a few times. This will likely increase soon. Shown below, it has been sequenced in the U.S. states of Texas, California and New York.
FY.3
On June 5, 2023, a sequence of FY.3 in China, shows some very concerning mutations.
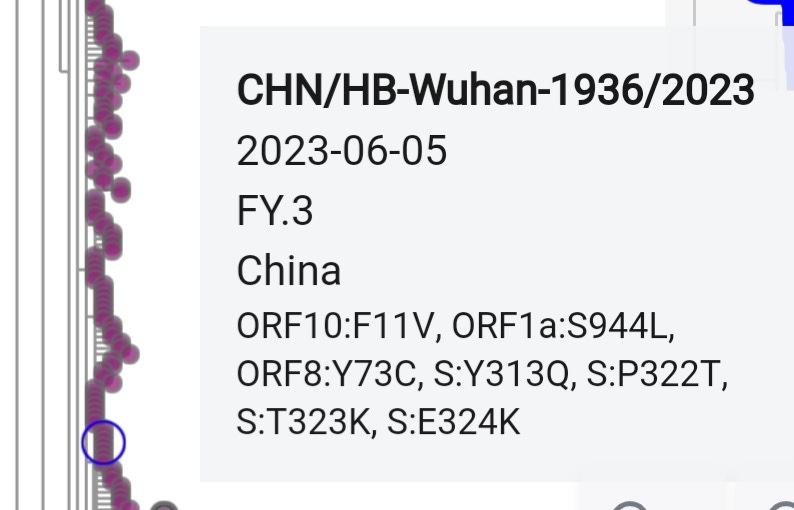
ORF8:Y73C
“Survival analysis of mutations in the SARS-CoV-2 genome revealed 27 of them were significantly associated with higher mortality of patients. Most of these mutations were located in the genes coding for the S, ORF8, and N proteins.”
“ORF8:Y73C, ORF8:R52I, and ORF8:Q27*, which affect the PF12093 (betacoronavirus NS8 protein) motif, allowing SARS-CoV-2 ORF8 to form unique large-scale assemblies that potentially mediate unique immune suppression and evasion activities [65,66];”
“ORF1ab:I2230T, does not affect any known motif, but it is significantly associated with patient higher mortality.”
ORF10:F11V
F11L 87% Deleterious
F11S 87% Deleterious
F11V ??
A study published on 1 January 2022: “Emergence of unique SARS-CoV-2 ORF10 variants and their impact on protein structure and function” The SARS-CoV-2 open reading frame 10 (ORF10) protein interacts with multiple human proteins CUL2, ELOB, ELOC, MAP7D1, PPT1, RBX1, THTPA, TIMM8B, and ZYG11B expressed in lung tissue. Mutations and co-occurring mutations in the emerging SARS-CoV-2 ORF10 variants are expected to impact the severity of the virus and its associated consequences.”
“Among all these residue positions, only the mutations at positions 11 and 16 in ORF10 variants in North America were predicted to be deleterious.” Just in case you weren’t sure, deleterious means causing harm or damage.
A study published: 29 November 2021, “SARS-CoV-2 ORF10 suppresses the antiviral innate immune response by degrading MAVS through mitophagy”
“our results indicate that SARS-CoV-2 ORF10 promotes viral replication via degradation of MAVS.”
“The function of ORF10, which is uniquely expressed in SARS-CoV-2, was unknown. In the present study, we found that SARS-CoV-2 ORF10 induces mitophagy to degrade MAVS by binding to NIX, thus blocking MAVS-mediated antiviral signaling and promoting viral replication.”
“Viral antagonism of the host innate immune response is critical for viral replication. In this study, we showed for the first time the function of SARS-CoV-2 ORF10 in suppressing the innate immune response. The expression of ORF10 inhibited the expression of IFN-β and ISGs and the transcription of IFN-α1 and IFN-β mRNAs. The RLR signaling pathway plays an important role in identifying infection with RNA viruses and regulating the cellular innate immune response. By screening adapter proteins in the RLR signaling pathway, we identified MAVS as the target via which ORF10 suppresses the IFN-I signaling pathway. At present, the negative posttranslational regulation of MAVS is thought to be achieved mainly by K48-linked ubiquitination [35], blockade of signal transduction, and autophagy [46]. In ORF10-expressing HeLa cells, treatment with CQ or Baf A1 but not MG132 reversed the ORF10-mediated inhibition of MAVS expression, indicating that ORF10 degrades MAVS through the autophagy pathway.”
“Autophagy is a critical degradation process in all eukaryotes that mediates the elimination of harmful components [47], while the innate immune system is the first line of defense against invading pathogens [48]. Innate immunity and autophagy are inextricably linked and reciprocally regulated.”
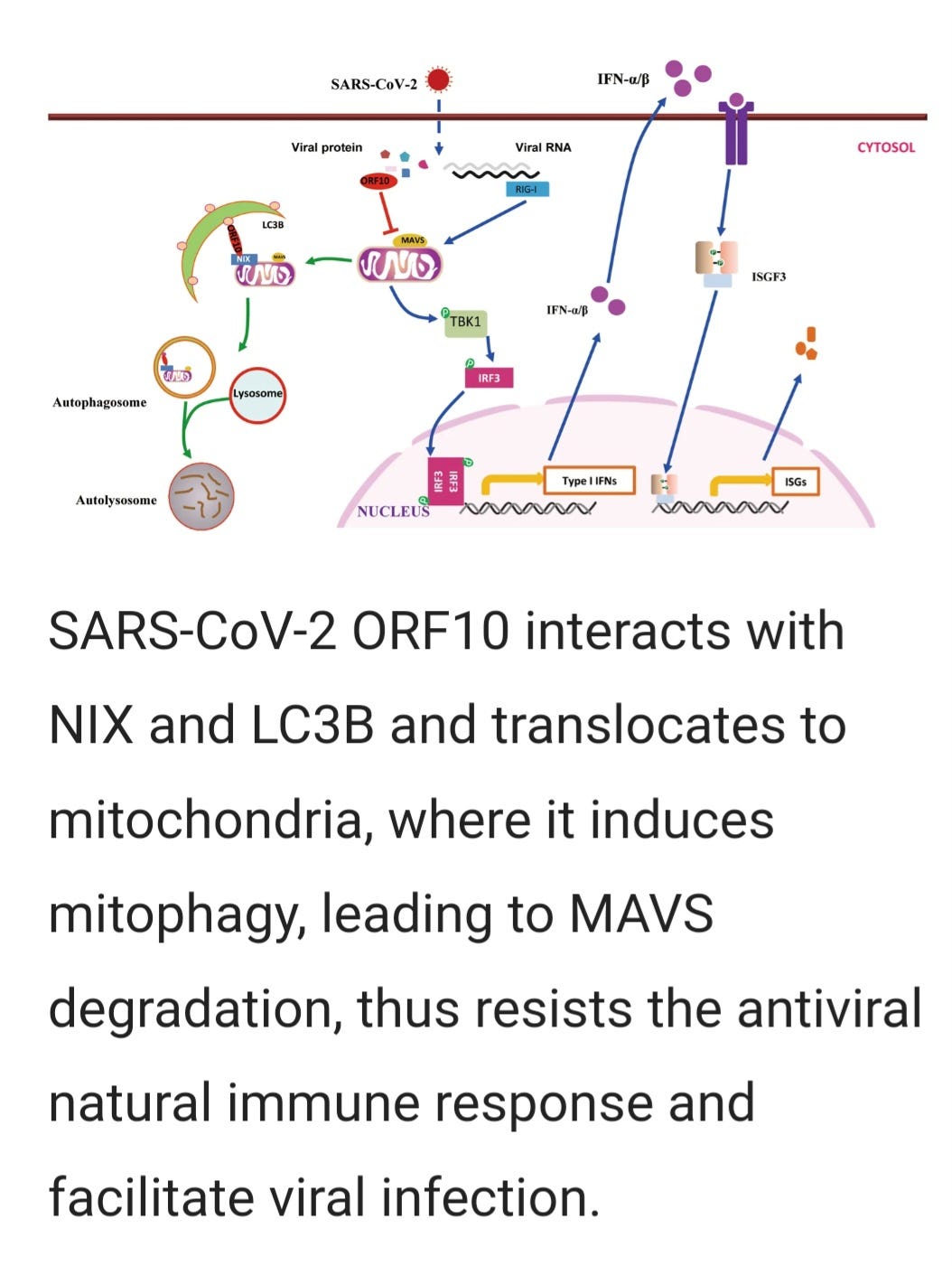
“SARS-CoV-2 ORF10 protein abrogates antiviral innate immunity and facilitates viral replication (Fig. 7). Our findings indicate that ORF10 interacts with NIX and LC3B to induce mitophagy, subsequently leading to blockade of MAVS-mediated antiviral signaling. The findings of this study provide a new direction for the study of the molecular mechanism by which SARS-CoV-2 resists antiviral innate immunity.”
3. “SARS-CoV-2 ORF10 impairs cilia by enhancing CUL2ZYG11B activity”
This study was published June 08 2022
“SARS-CoV-2 ORF10 alone results in cilia-dysfunction-related phenotypes, and the ORF10 expression in primary human nasal epithelial cells (HNECs) also caused a rapid loss of the ciliary layer. Our study demonstrates how SARS-CoV-2 ORF10 hijacks CUL2ZYG11B to eliminate IFT46 and leads to cilia dysfunction, thereby offering a powerful etiopathological explanation for how SARS-CoV-2 causes multiple cilia-dysfunction-related symptoms specific to COVID-19.”
These studies are telling us that there is a good chance the mutation in ORF10 could make this variant more dangerous and one that we will continue to follow closely.
The latest variants are the most immune evasive and suppressive to date. That means the risk of persistent infections and Long COVID symptoms will increase. This is a crisis that demands collective action and change. Long COVID is not an isolated struggle; it reverberates through every corner of society. The impact is felt in families, workplaces, healthcare systems, and beyond. It is a preventable catastrophe that requires a united effort from all of us to alter its course.
We must work Together Against COVID Transmission.
Let us know what you're seeing or experiencing where you are or any other insights you may have.