



COVID Update April 21, 2024: Don't Get Blindsided: Tracking COVID's Next Move as KS.1 Surges from 3% to 19% Prevalence in Canada
Staying Vigilant: Navigating Risks Despite a Decrease in Prevalence

COVID is far from over. Despite the progress made, it continues to spread at alarming rates, especially when compared to other respiratory pathogens. Adding to the concern is the emergence of the highly mutated KP.2 variant, which now constitutes roughly 10% of global cases, although this estimate is conservative due to limited genomic sequencing data. We're still learning about its impact, but it's clear that it's outcompeting JN.1, indicating its potential for increased transmissibility or immune evasion.
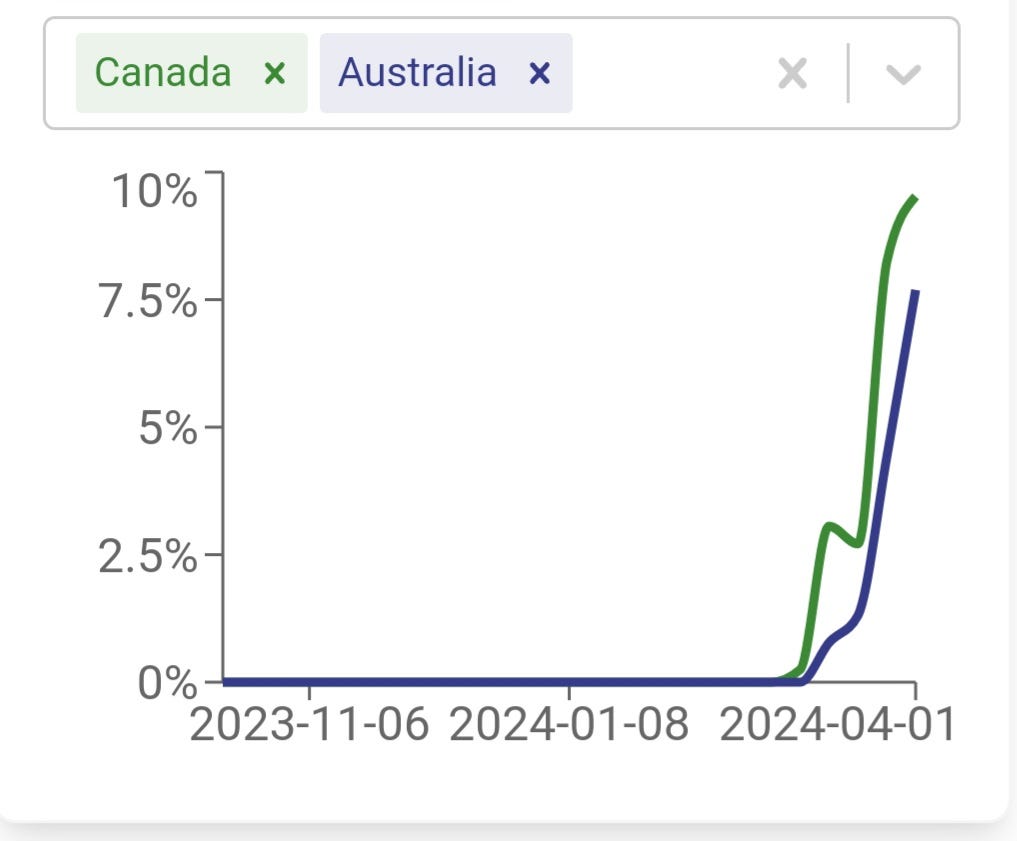
Taking a closer look at countries like the U.S., and Canada, and using worldwide sequencing data, we're seeing KP.2, along with variants like KP.3 and the newer KS.1, gaining ground. For instance, KS.1 has shown a significant jump in Canada's data, from 3.45% to 19.7% in just one week. While this rapid increase needs more observation over time, it's definitely a cause for concern. Understanding the mutations driving these variants is crucial to assessing their threat level.
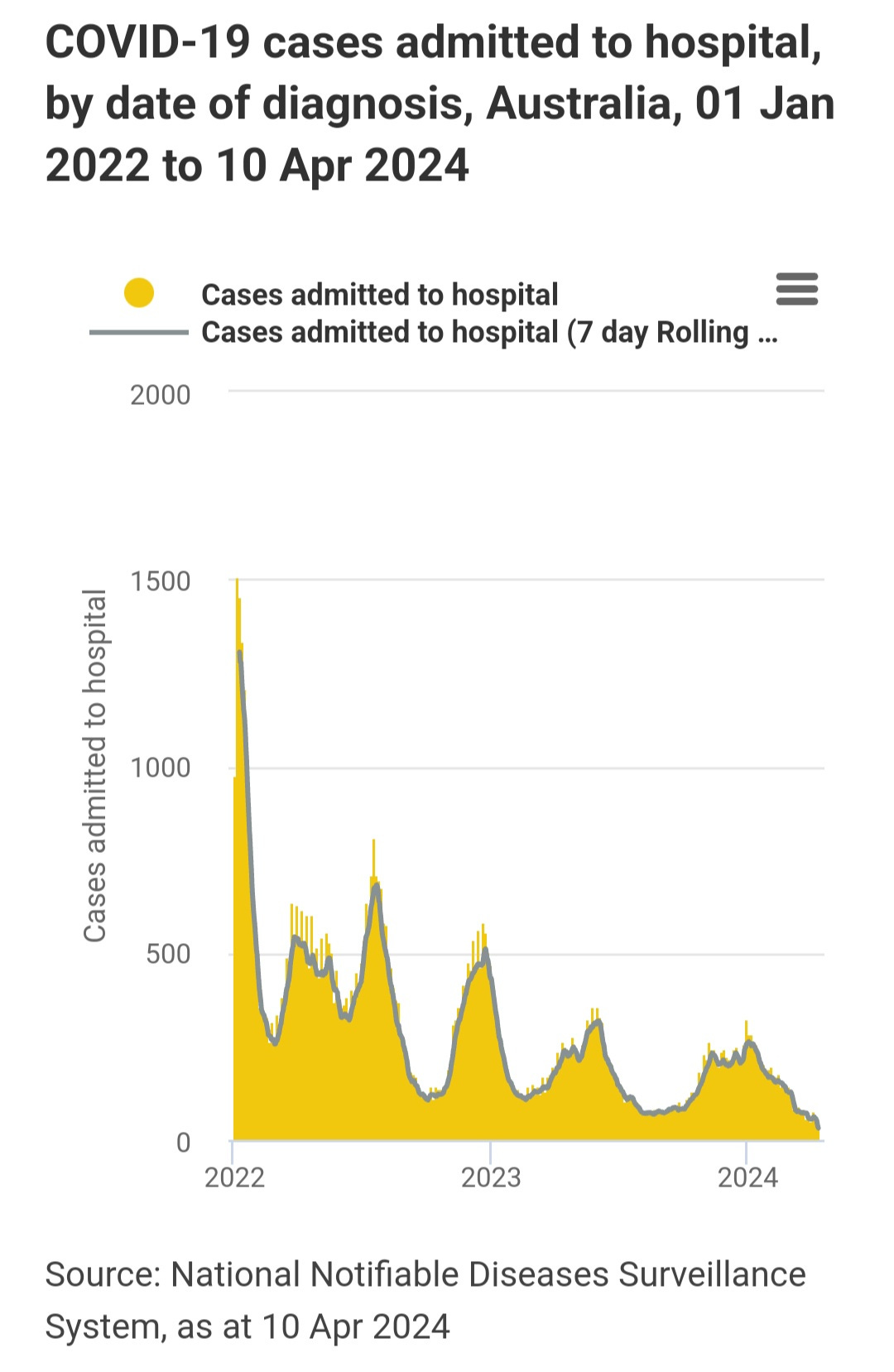
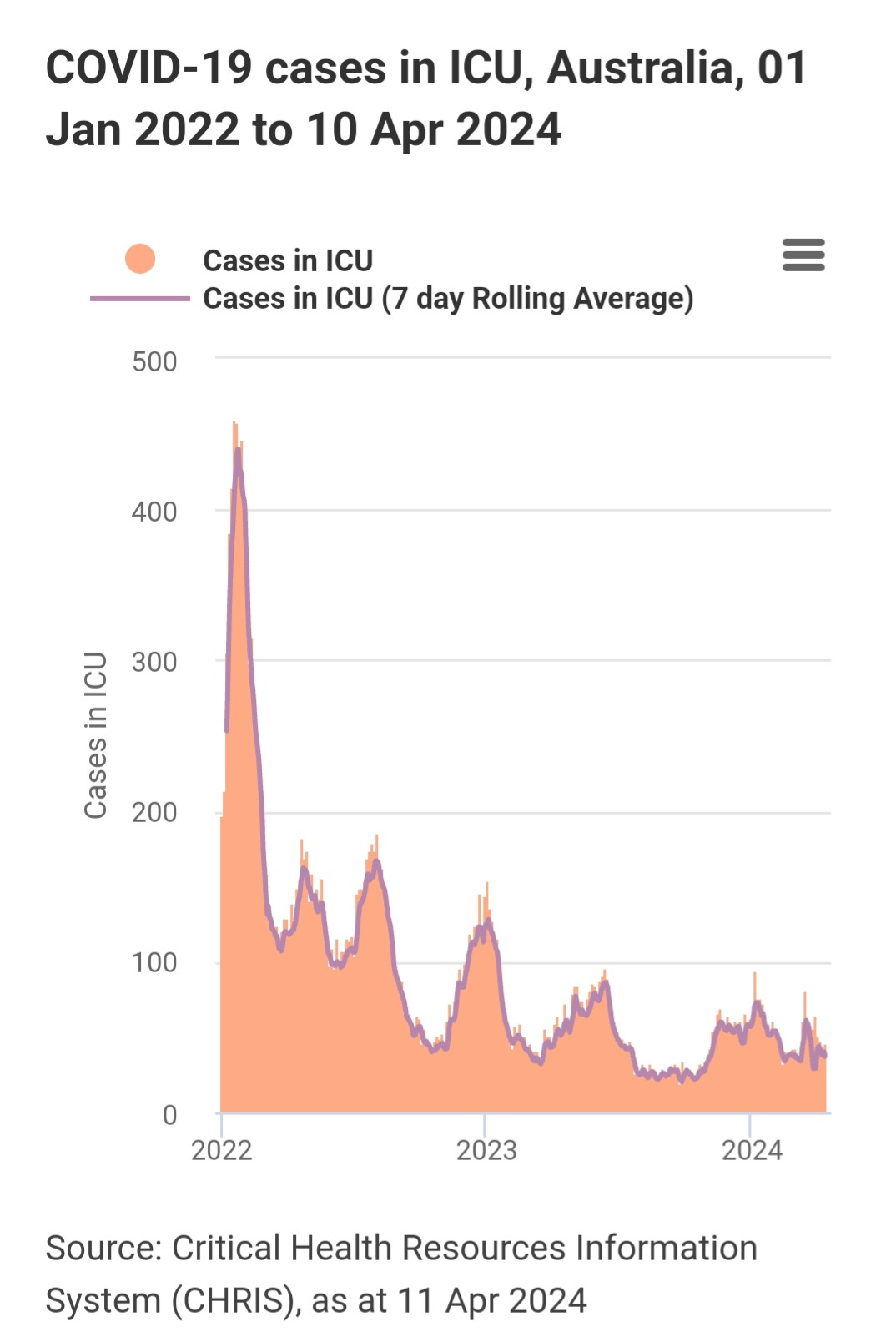
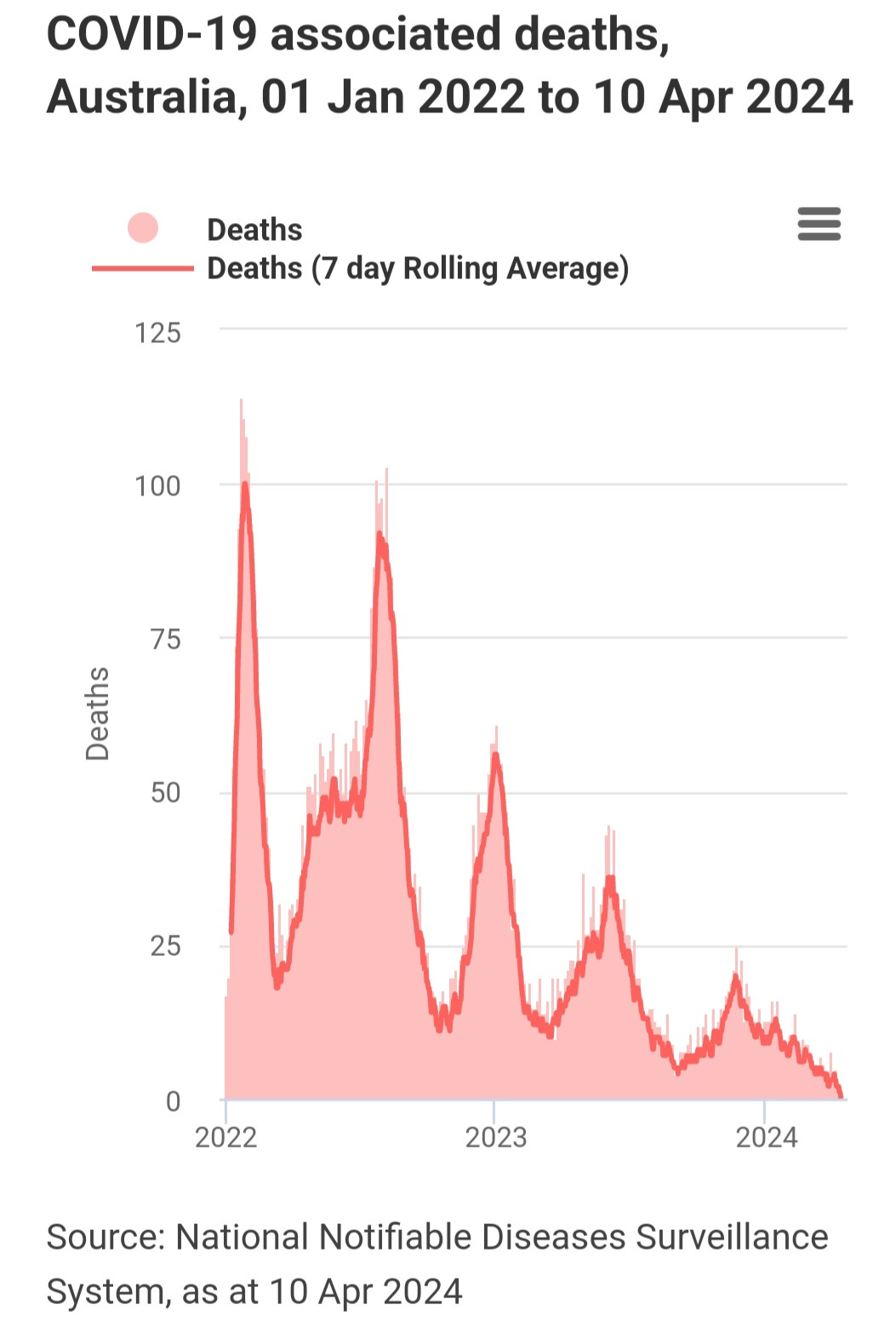
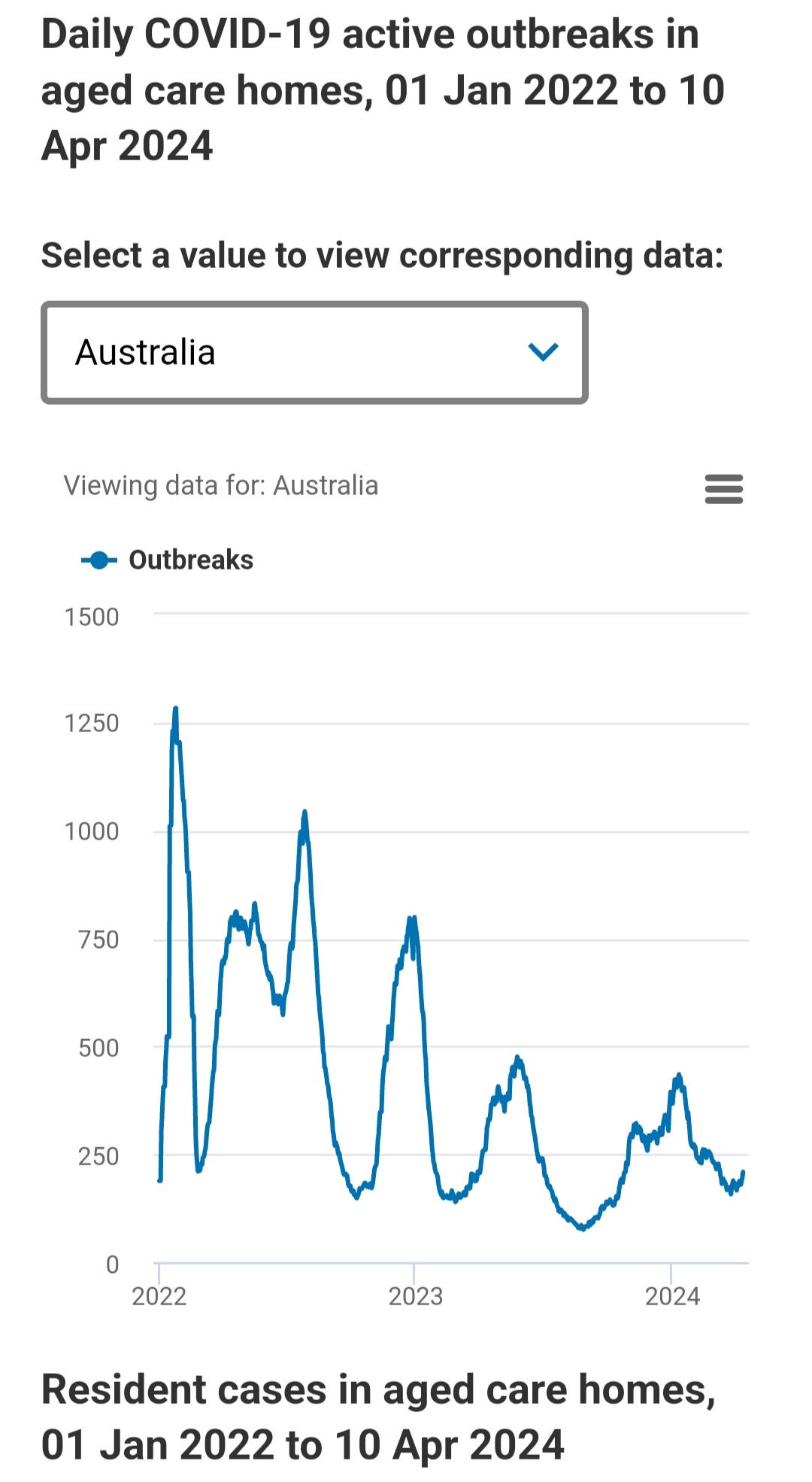
We will take a look at the hospitalizations, deaths, and wastewater prevalence in the U.S., Australia, Germany, and a couple of other countries, but overall hospitalizations and deaths are declining but this is also deceiving. There is a slight uptick in care home outbreaks in Australia, one of the only countries still tracking care home outbreaks.
Unfortunately, there's a lack of awareness about these variants and their ability to evade and attack the immune system, leading to systemic infections with little to no initial symptoms. Weakened immune systems become more susceptible to secondary infections from opportunistic viruses, bacteria, and fungi. The symptoms associated with the secondary infections may be the first signs of a current or recent COVID infection. While the odds of new COVID infections have decreased compared to the past six months, they're still occurring widely, and new variants are on the rise.
This update will delve into essential data and provide insights into what to anticipate in the coming months.
Stay Informed, Stay Empowered: Independent Coverage
By subscribing, you'll gain access to:
Unbiased reporting: We cut through the noise and deliver critical information you need to make informed decisions about your health.
In-depth analysis: TACT goes beyond headlines to uncover details and the true impact of COVID, Bird Flu, Monkeypox, and other emerging or evolving diseases.
Empowering insights: We translate complex scientific data into actionable knowledge, putting you in control of your well-being.
Support Independent Journalism - Subscribe Today!
Immediate access is available to paid subscribers. Your continued support means the world to us.
Keep in mind that this delay could be eliminated for free subscribers with just 120 more paid subscribers. Help us make this accessible without delay for everyone by becoming a paid subscriber today.
United States
The prevalence of U.S. wastewater is steadily declining and is expected to reach its lowest point of the year in the next month or two. Although significantly lower than the peak in January, with prevalence averaging between 20% to 30%, it's evident that the virus is still circulating widely.
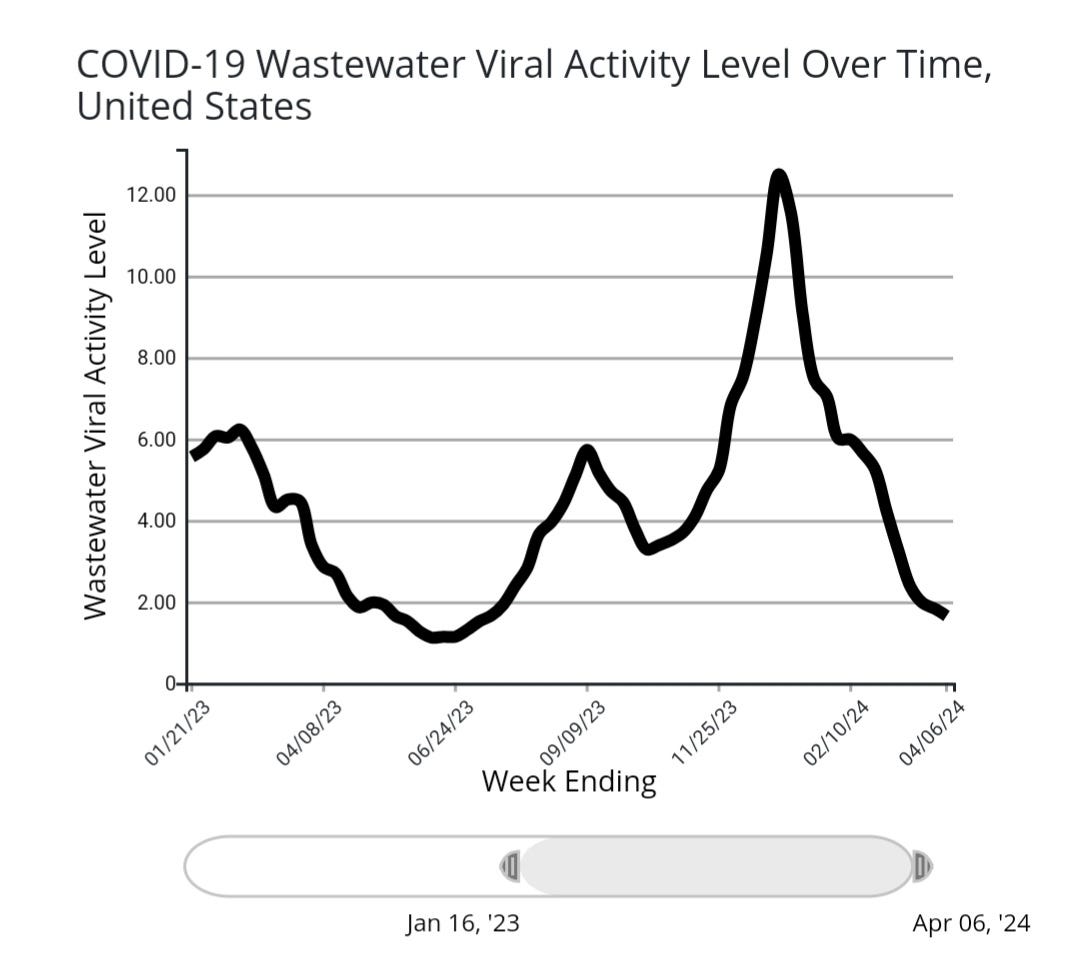
Biobot - Year over Year U.S. Wastewater prevalence
The wastewater prevalence in 2024 is now closely following that of 2023.
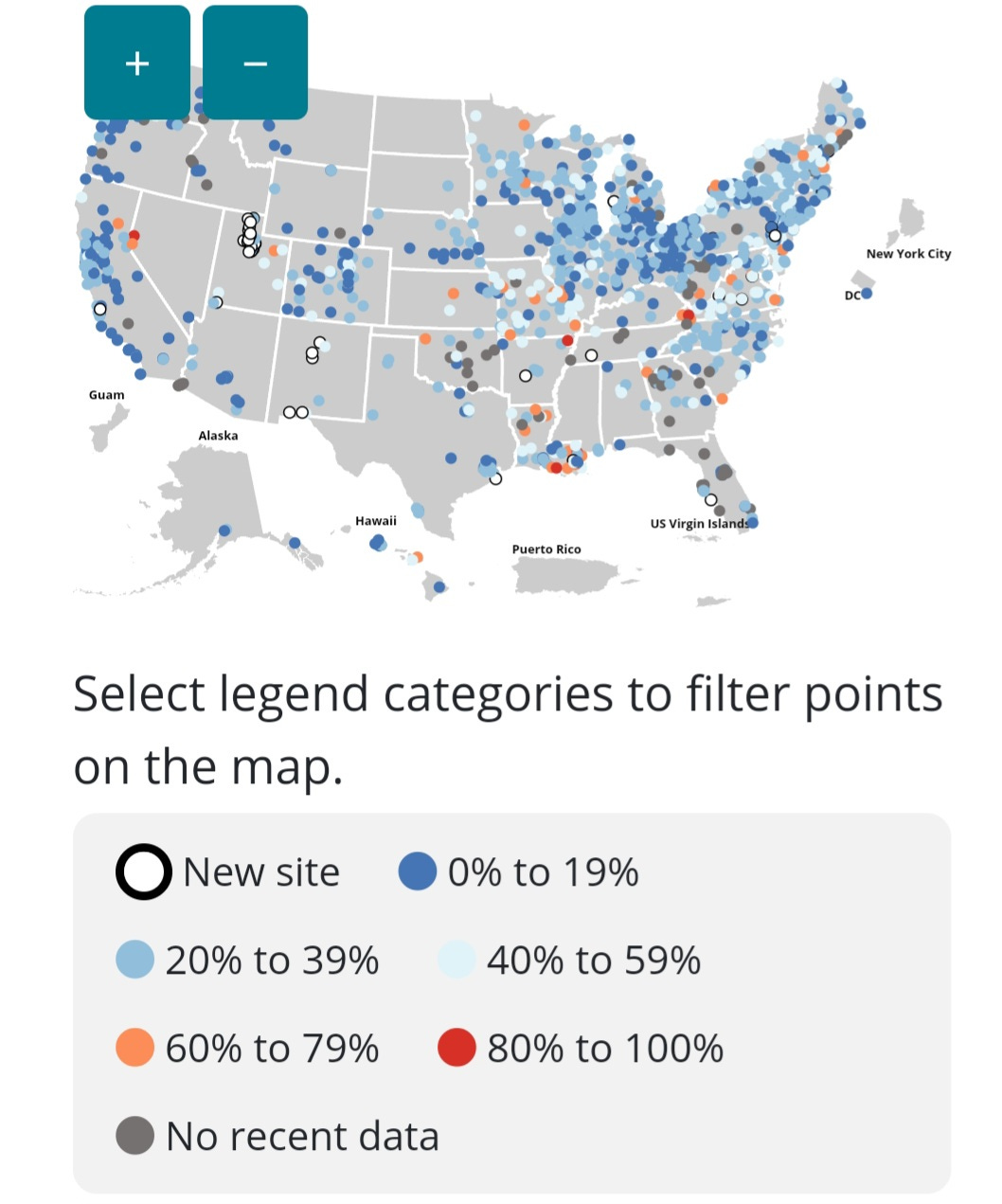
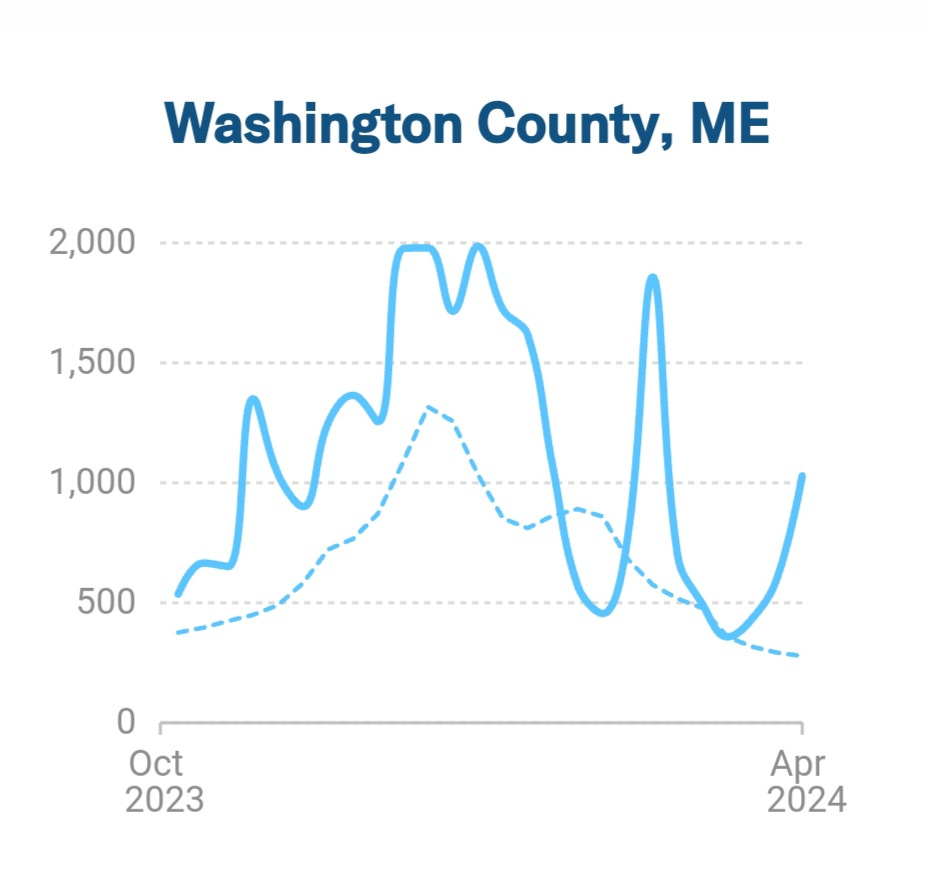
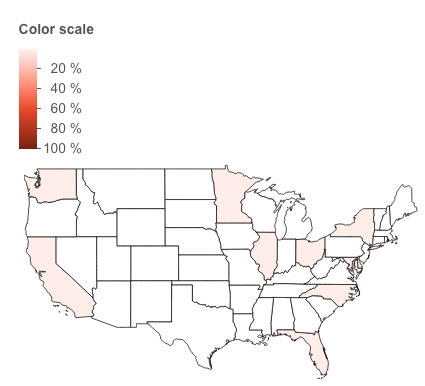
Hot Spots with Increasing Wastewater Prevalence



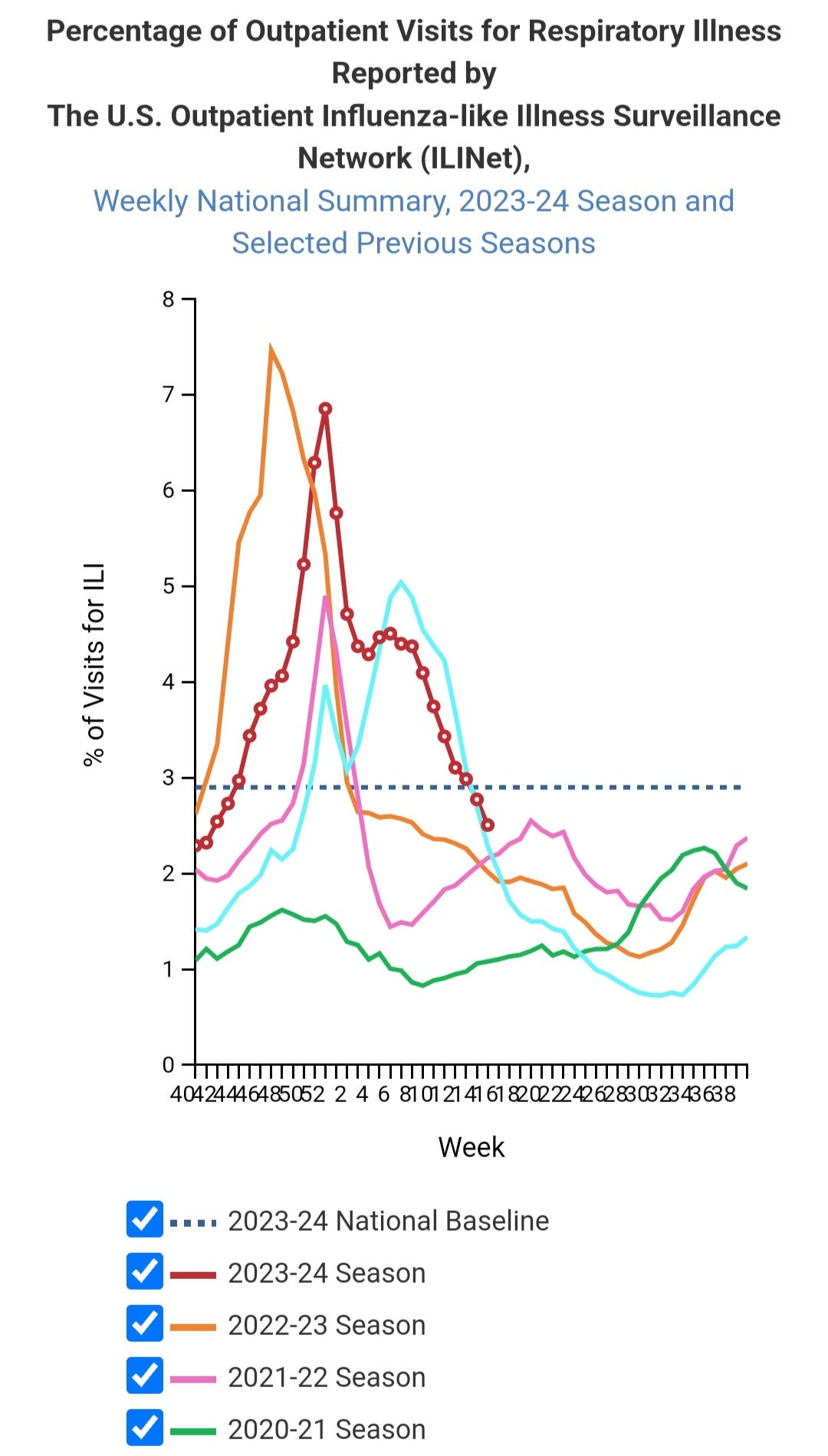
U.S. Outpatient Visits for Respiratory Illness
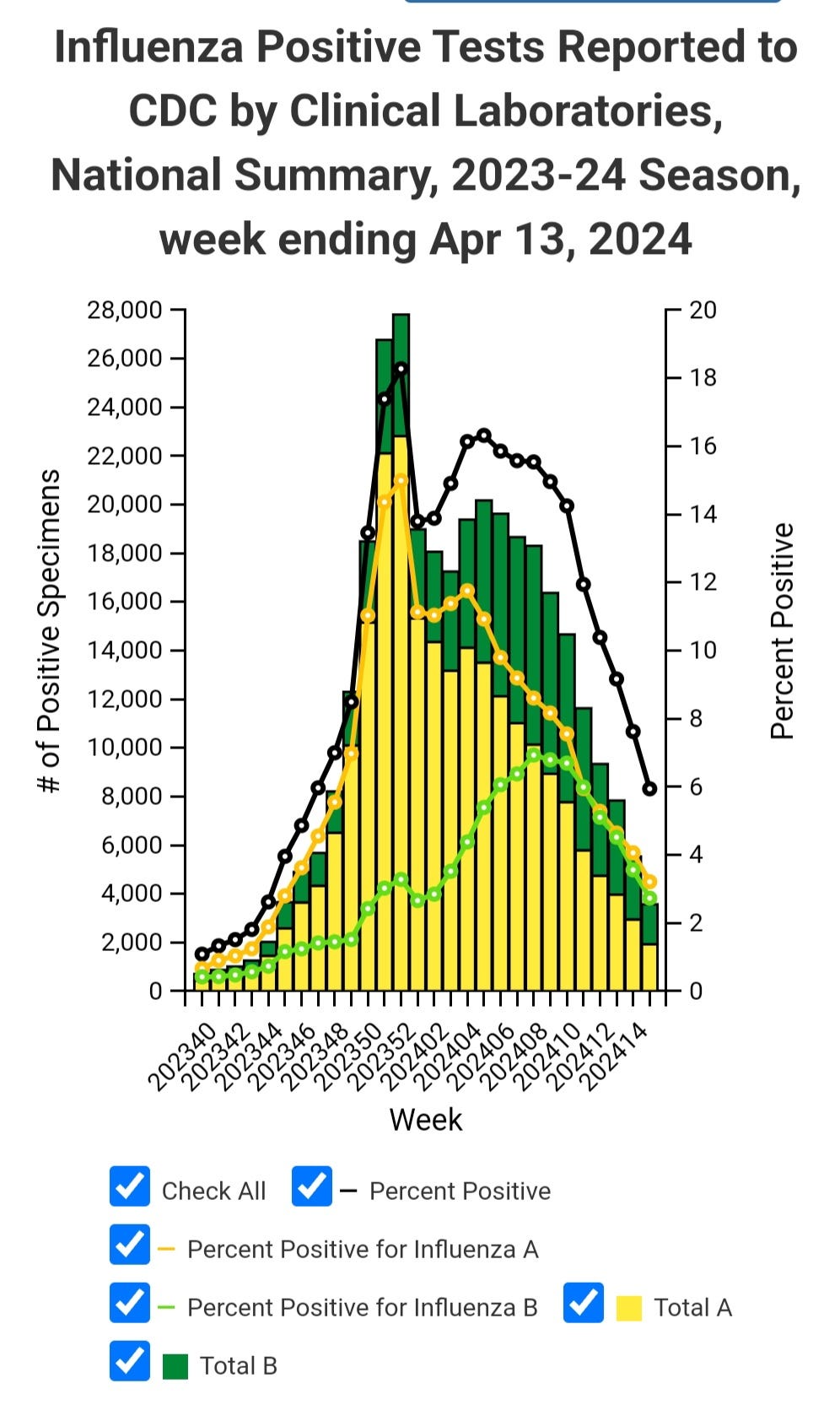
U.S. Influenza A and B is Decreasing
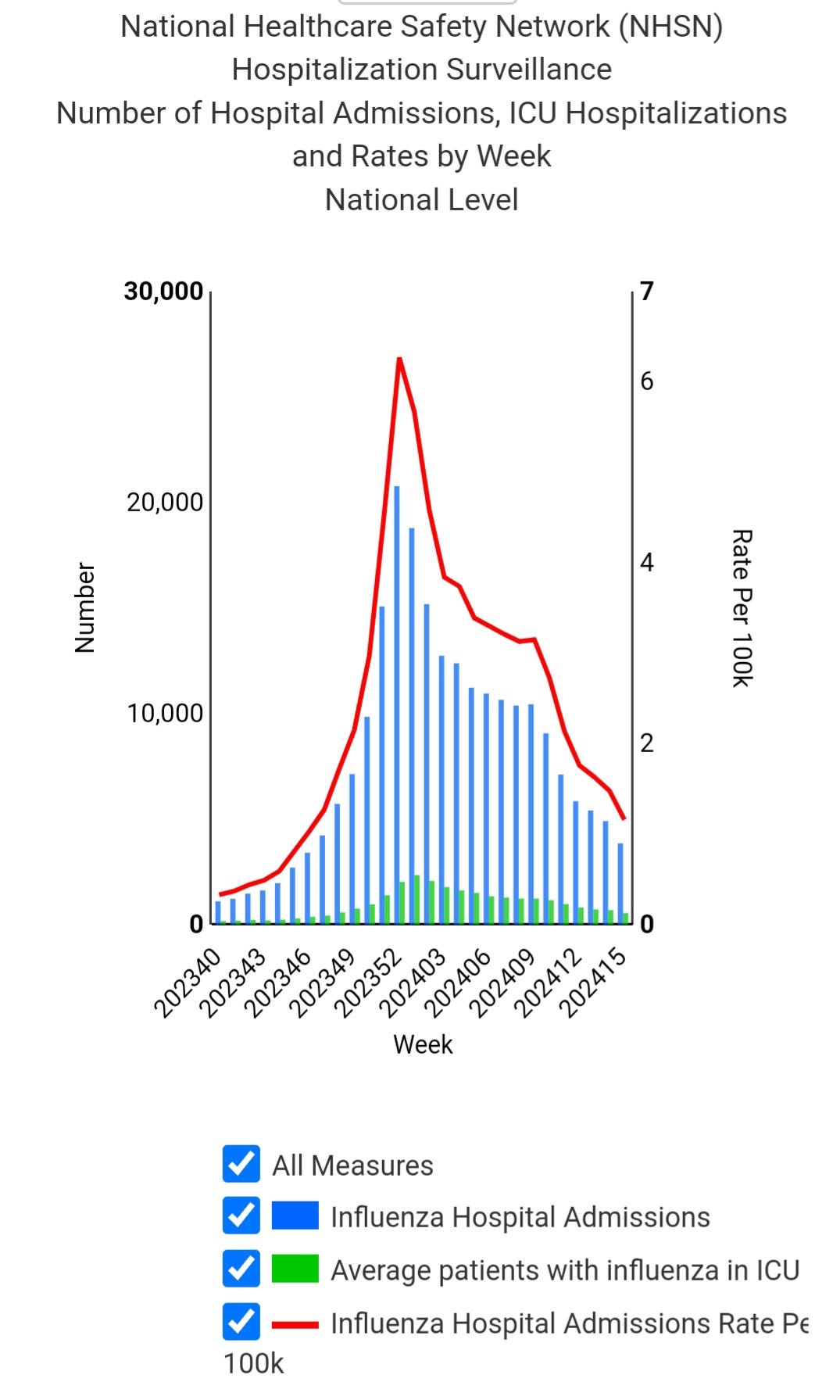
Influenza Hospitalizations Decreasing
Australia
Outbreaks in Australian Care Homes Ticking Up
Sweden Wastewater Data
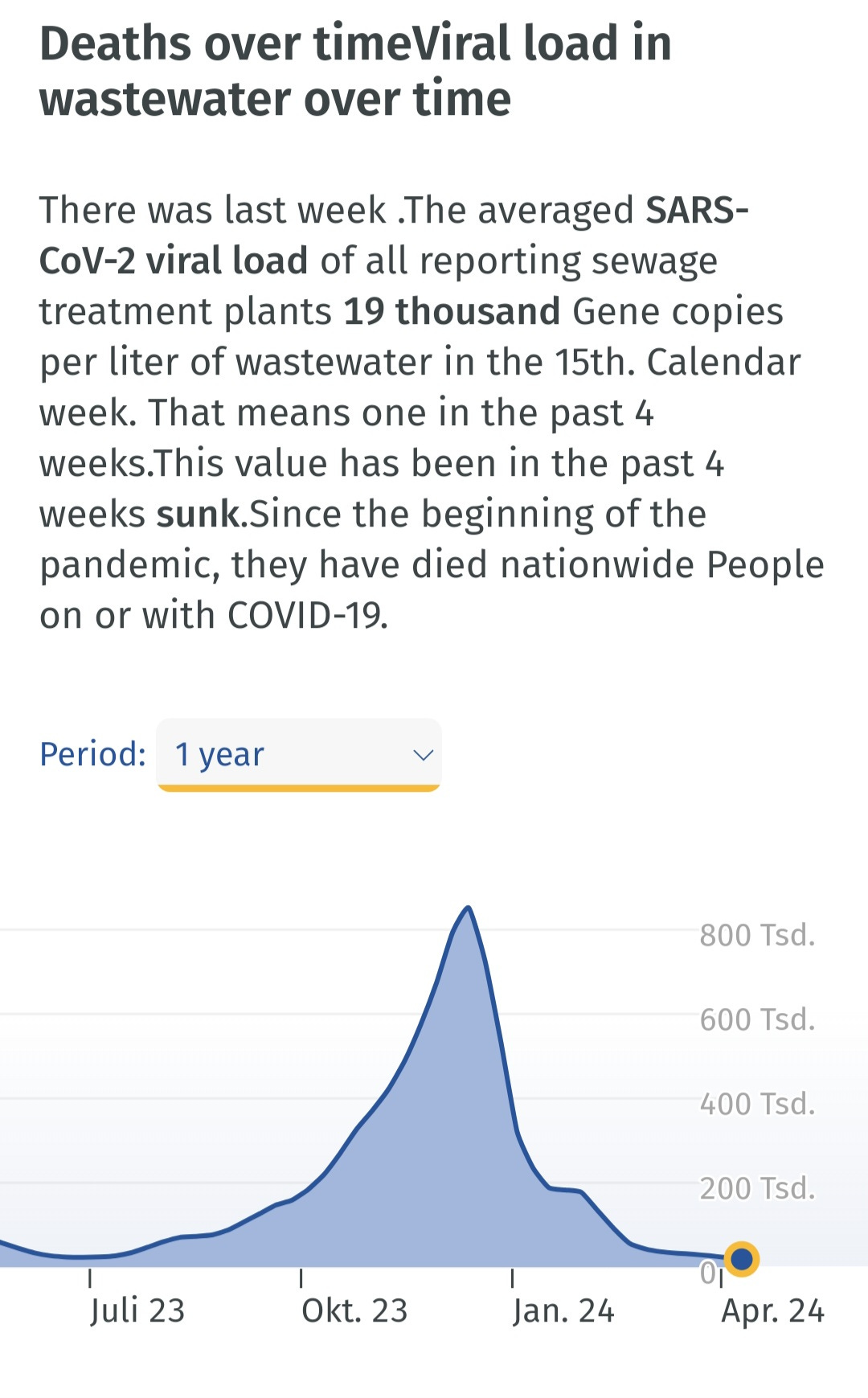
Germany Wastewater
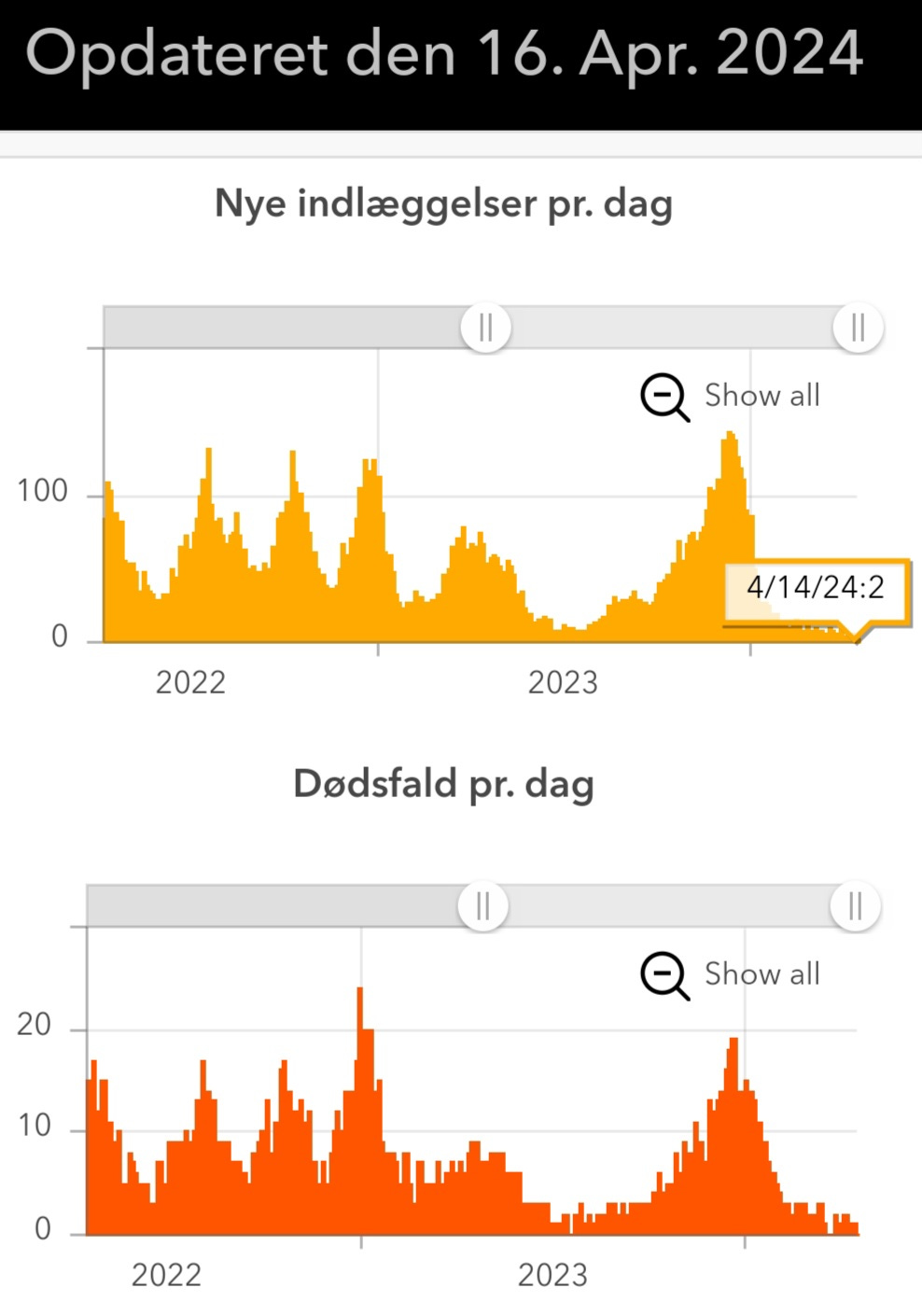
Denmark Hospitalizations and Deaths
COVID Variants
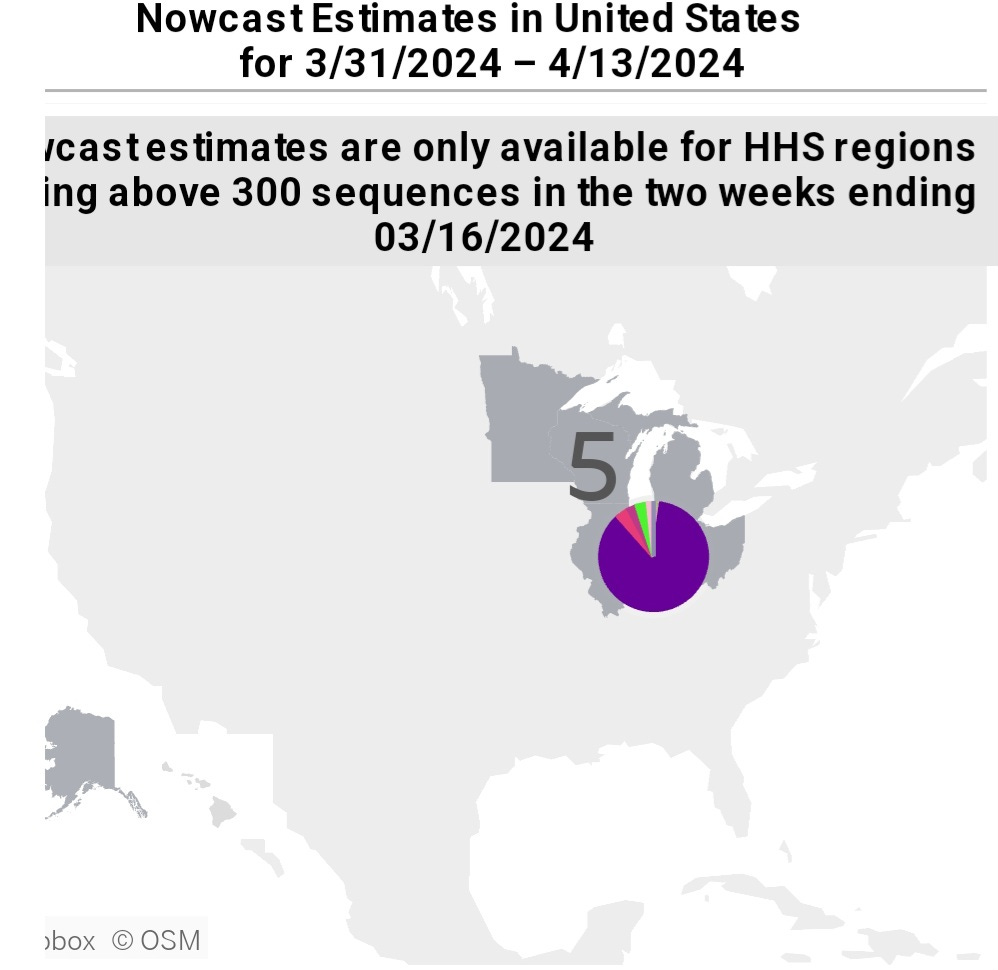
U.S. CDC Variant Proportions
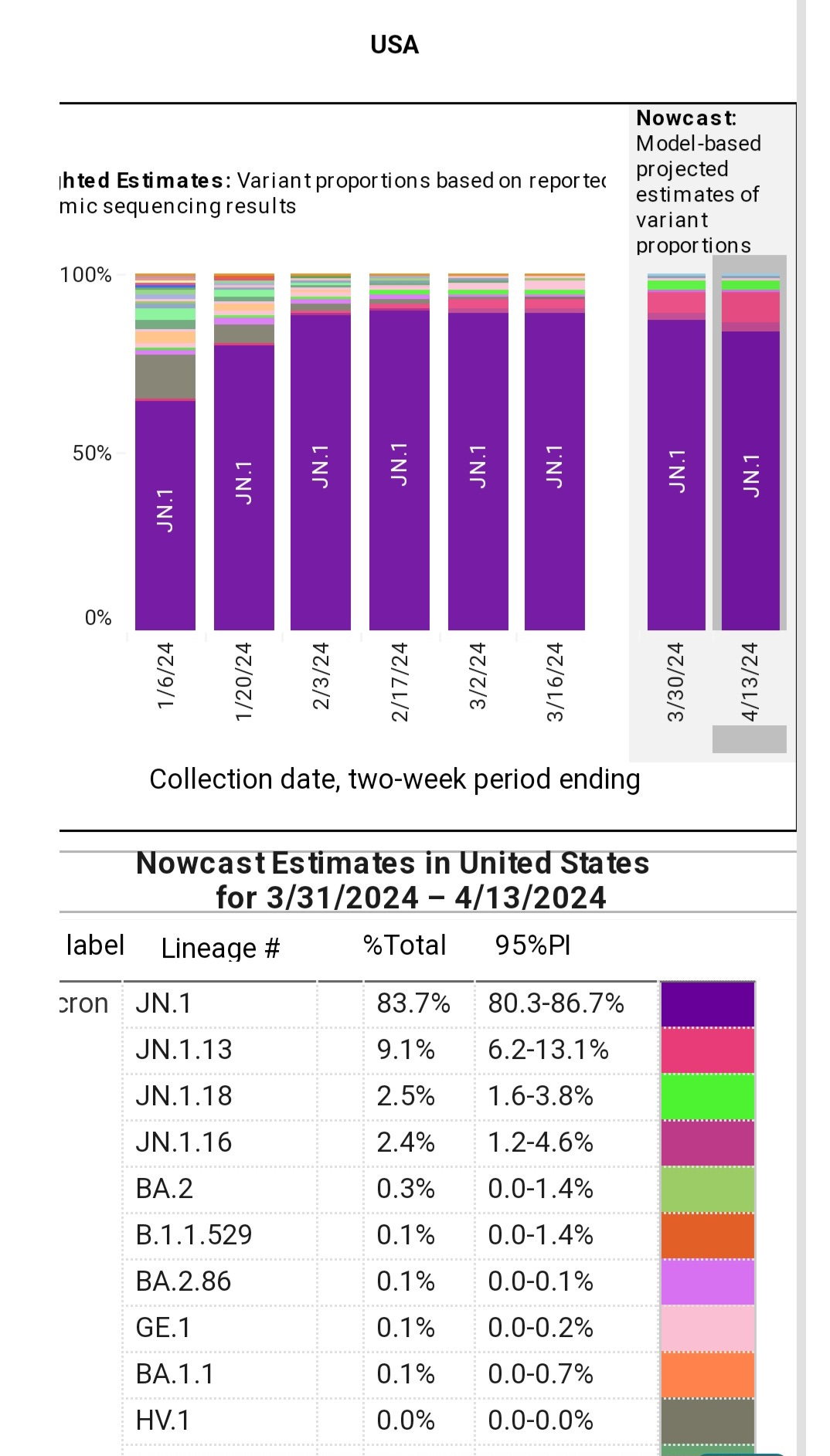
This sadly only represents one region reporting data because the other regions had less than 300 sequences in the two weeks ending March 16, 2024. In other words, we really can't properly assess the risk.
Canada
Variant Proportions
KP.2 grew from 6% (3/31/2024) to 9% (4/7/2024), while KP.3 decreased from 10% to 4.5%. KS.1, short for JN.1.13.1.1, has a big jump increasing from 3.45% on 3/31/2024 to 19.7% as of 4/7/2024. We will have to keep a close on on KS.1.

COVID Variants, KP.2, KP.3, and KS.1
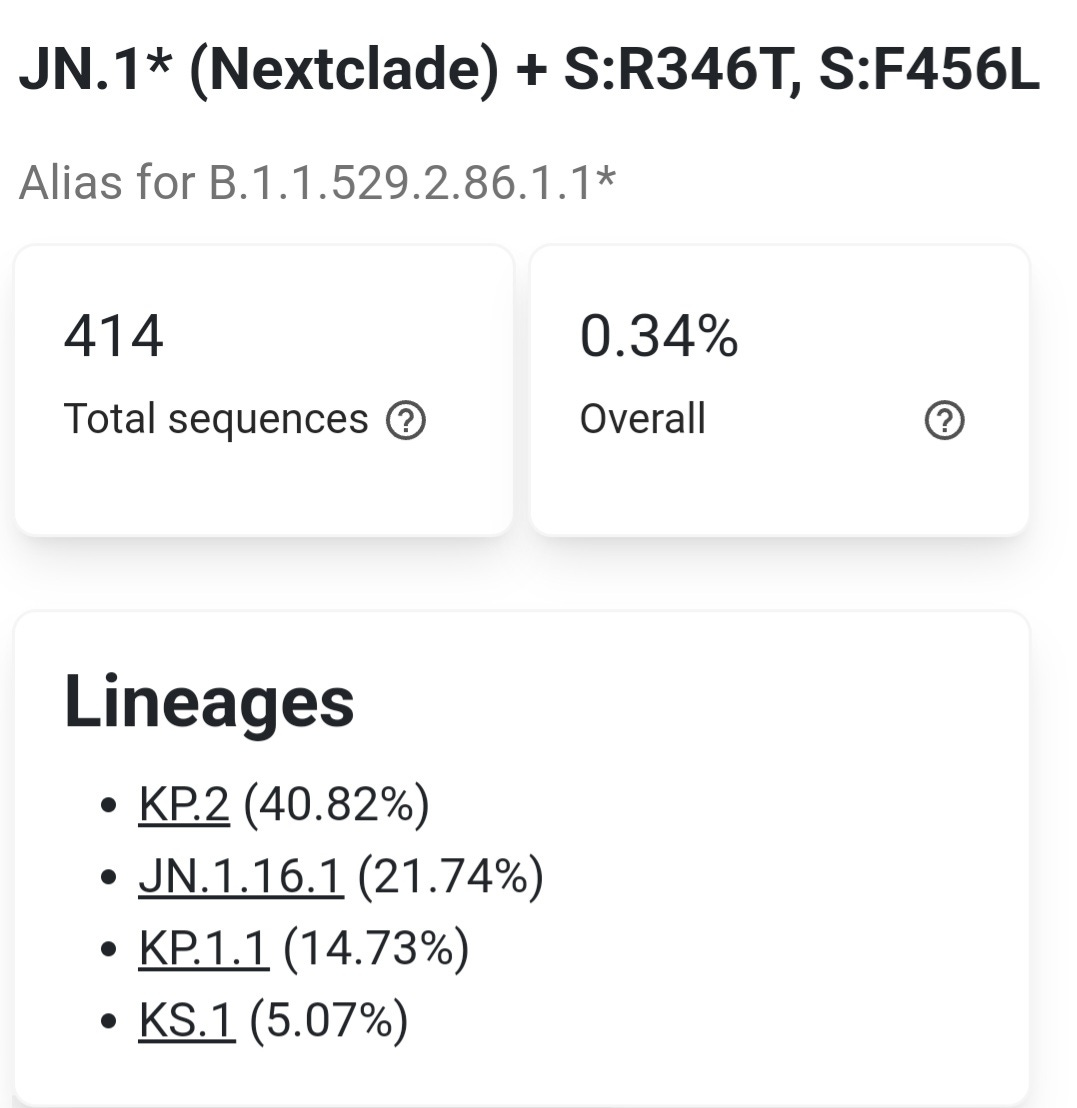
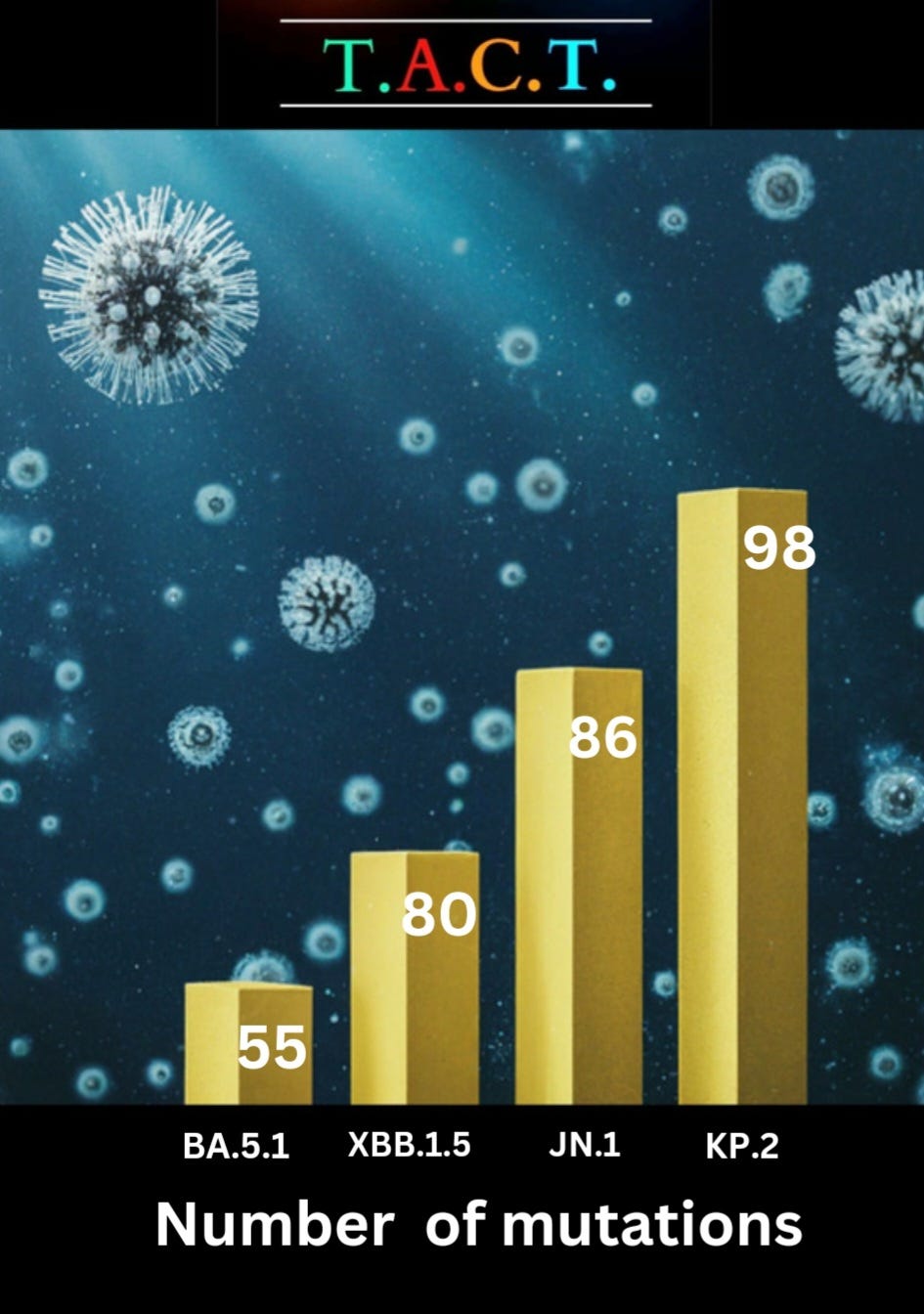
KP.2 and the number of mutations compared to earlier variants.
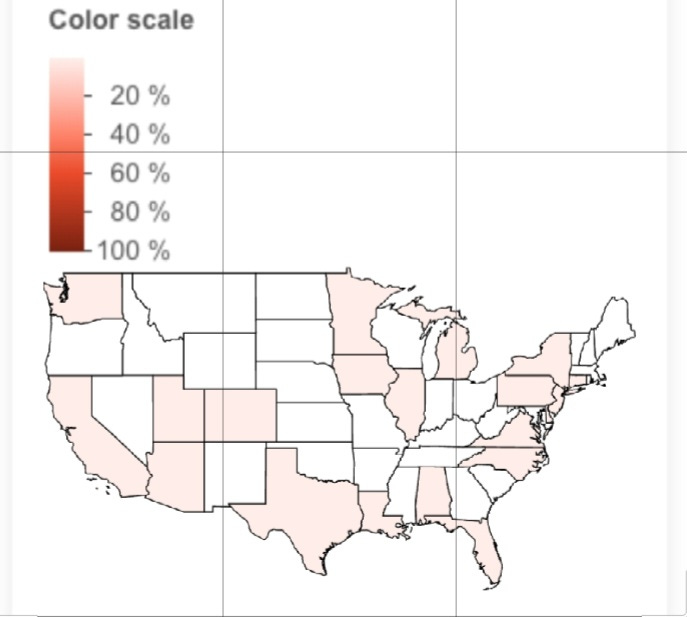
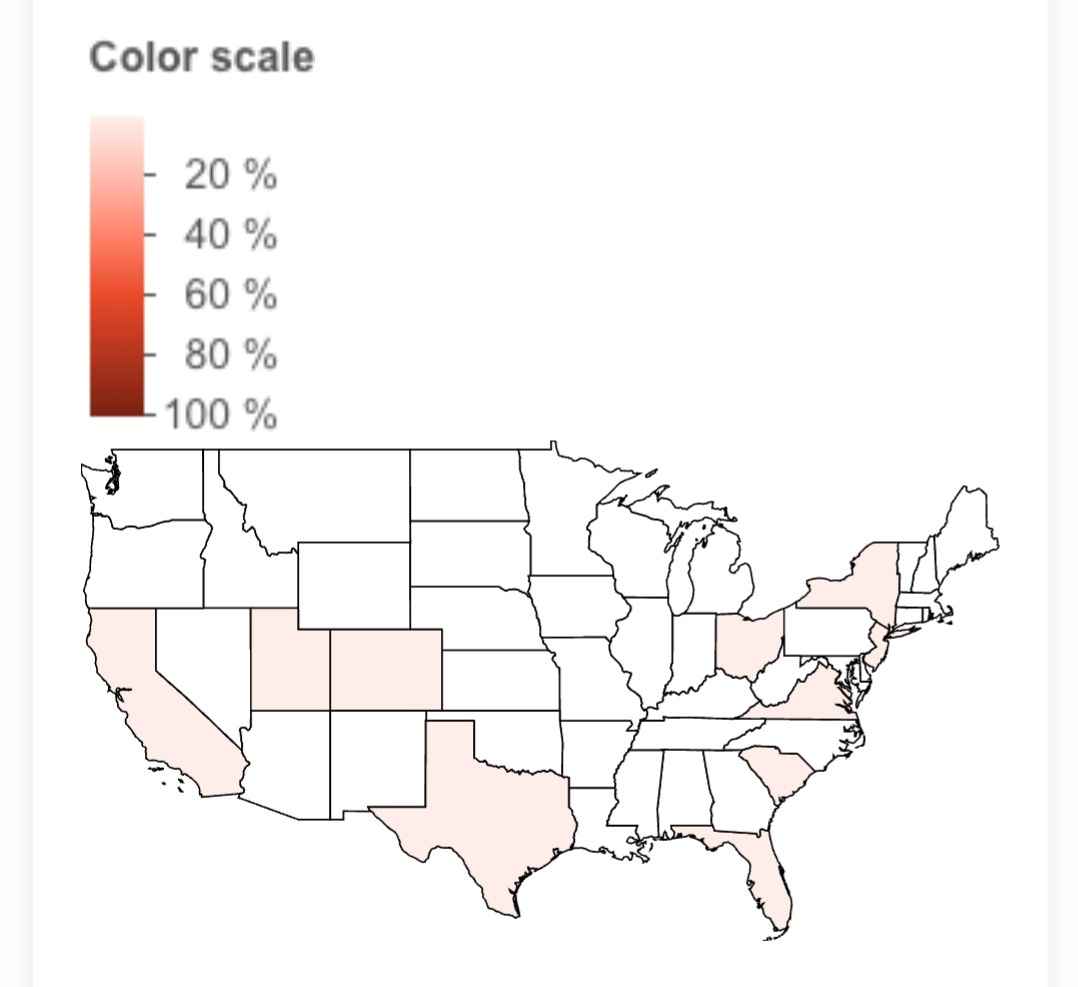
KP.2 in the U.S.
KP.2 has been sequenced in at least 19 states and 12 countries. It has likely expanded to far more countries and states than current data is reporting.
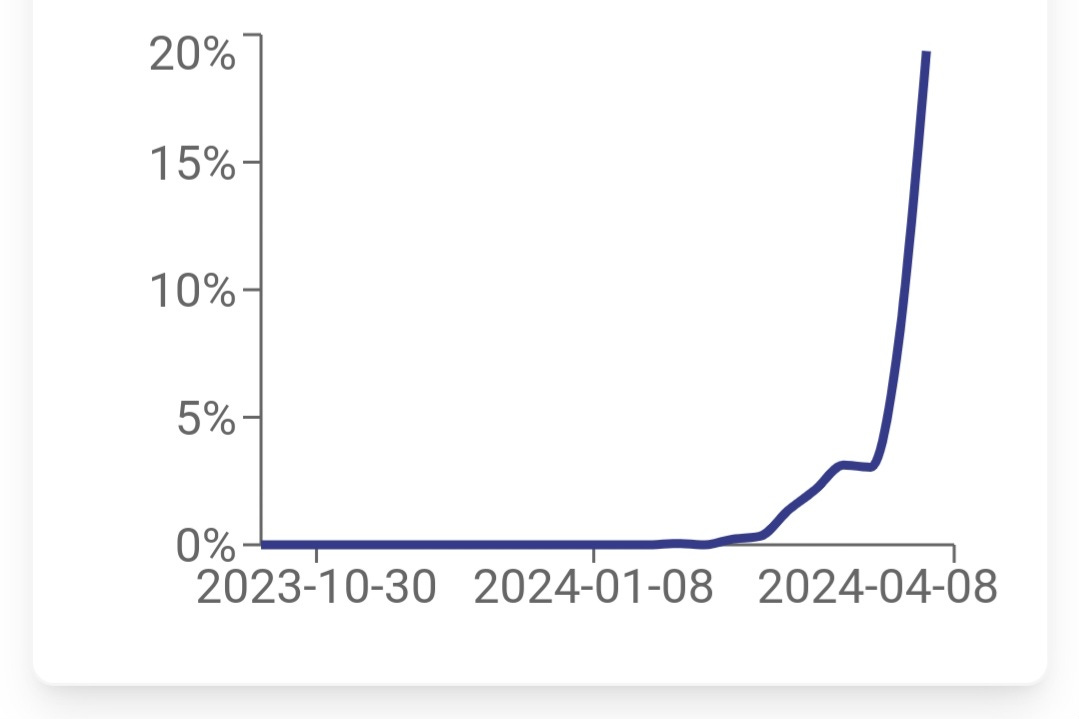
The graph below shows the growing prevalence of KP.2 in the U.S.
KP.3 (JN.1.11.1 plus S:Q493E)
KP.3 has 8 fewer mutations than KP.2 but it has a new mutation in the spike that KP.2 doesn’t have. That is the S: Q493E which involves a substitution of the amino acid glutamine (Q) with glutamic acid (E). The mutation has been primarily observed in the now-outdated lineage AY.49, a sublineage of Delta. Importantly, the Q493E mutation is associated with resistance to monoclonal antibody therapies like bamlanivimab and etesevimab. (1) This means these treatments may be ineffective against viral strains carrying this mutation.
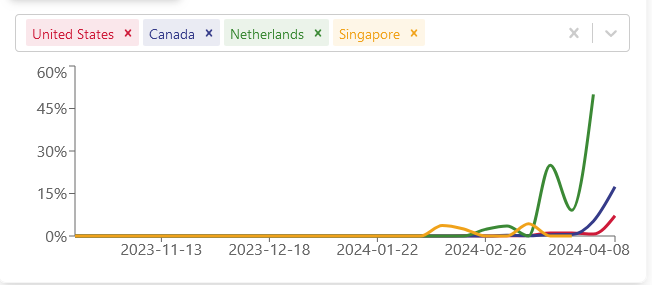
Sequencing has revealed the highest numbers KP.3 in Canada and Thailand, while the highest numbers of KS.1 were found in the Netherlands, followed by Canada.
In the last 10 days, there have been 210 sequences of the KP.2 variant and 73 of KP.3. The higher growth advantages of KP.3 and KS.1 suggest they may eventually surpass KP.2. However, it's still too early to confirm this.
Everyone should remain vigilant for individuals exhibiting new symptoms or experiencing infections from bacteria, viruses, or fungi that they wouldn't typically be susceptible to. These symptoms could serve as early indicators of a new COVID infection.
KS.1 (JN.1.13.1.1 or BA.2.86.1.1.13.1.1)
Take a moment to reflect on how far BA.2.86 has evolved since writing the update on Nov 29, 2023. You can read that article below.
BA.2.86's Stealthy Rise to Dominance - Also Known as the Pirola Variants - Increased Immune Evasion and Suppression! Analyzing the BA.2.86 Surge Around the World

The Pirola variant family, represented by BA.2.86, is rapidly expanding its presence, approaching an estimated 38% prevalence globally. This swift rise is notably displacing the XBB descendants. Before delving into the details of this trend, it's crucial to grasp that the immunity previously acquired against the XBB variants, commonly present in most individuals, is likely to be surpassed. This sets the stage for a significant increase in reinfections. Several recent studies provide in-depth insights into the mutations and evolutionary path of the BA.2.86 variants, showcasing their ability to outcompete other Omicron variants through heightened immune suppression.
KS.1 (JN.1.13.1.1 or BA.2.86.1.1.13.1.1) continued
KS.1 and KP.3 have the same number of mutations but here are some key mutational differences between KS.1 and KP.3
ORF1a:K680N (7.41%, 0.01) - Present in a portion of KS.1, absent in KP.3
ORF1a:D3897G (7.41%, 0.06) - Present in a portion of KS.1, absent in KP.3
ORF1a:E4388K (22.22%, 0.01) - Present in a portion of KS.1, absent in KP.3
ORF1b:P2612S (7.14%, 0.06) - Present in a portion of KS.1, absent in KP.3
S:F59S (100.00%, 0.04) - Present in all KS.1, absent in KP.3
S:V642A (14.29%, 0.10) - Present in a portion of KS.1, absent in KP.3
S:A1087S (100.00%, 0.04) - Present in all KS.1, absent in KP.3
Interestingly, F59S isn’t found in KP.2, JN.1, or XBB.1.5, and the search hasn’t turned up any papers on how this could impact the situation. TACT will keep you updated on this as more information becomes available.
TACT’s Overview
While the odds of a new COVID infection are much lower compared to the prior six months, new infections are still widely occurring. The next month or so presents the most opportune moment for individuals to schedule any previously postponed doctor or dental appointments. However, it's essential to remain vigilant as highly mutated variants with greater immune evasion capabilities are becoming more prevalent.
Sometime in June, we will likely see one or more of these newer variants displacing JN.1 completely. Combined with waning immunity after JN.1 infections, we will see the overall prevalence going back up from mid-June through late August.
COVID continues to pose significant health risks, manifesting as an increasingly efficient airborne immunosuppressive disease that accelerates epigenetic aging and causes dysfunction in various bodily systems, including vascular, musculoskeletal, and cognitive functions. The virus can infiltrate and persist in multiple organs, including the brain and heart, leading to long-term damage. Each reinfection heightens the risks associated with these outcomes.
The risk of persistent infections leading to Long COVID is underscored by recent data indicating that 27 U.S. states have over 30% of individuals reporting Long COVID (symptoms lasting longer than 3 months). The ages consistently most impacted are 25 to 55. These are working-age adults who are more likely to be parents of school-age children.
While overall prevalence may remain relatively low over the next month, it's crucial to recognize that the threat posed by new variants and the associated risks of infection remain substantial. Notably, many initial symptoms may be mild or go unnoticed, despite the virus spreading throughout the body and brain. Some individuals may mount a robust T-cell response, protecting them from severe consequences, while others may develop long-term disabling conditions. Minimizing exposure risk is paramount in mitigating these dangers. Stay safe and stay informed.
Please share your thoughts, insights, and ideas by leaving a comment.
"Strategies to Avoid COVID and Other Respiratory Viruses"
”Prevention is the Best Medicine”
https://tactnowinfo.substack.com/p/strategies-to-avoid-covid-and-other
Interesting photograph at the top. I wouldn't have expected the suns corona to look quite like that.
Maybe some filtering effects here, but interesting nonetheless.
I guess KS.1 is a FLipper variant. FLippers could be making their move.