



Arcturus (XBB.1.16): 241% Increase in India and India is Taking Action. XBB.1.16 is in 25 Countries and 23 States. XBB.1.31: Is an 800% growth advantage possible?
Research on the mutation that might be driving the advantage in XBB.1.31.

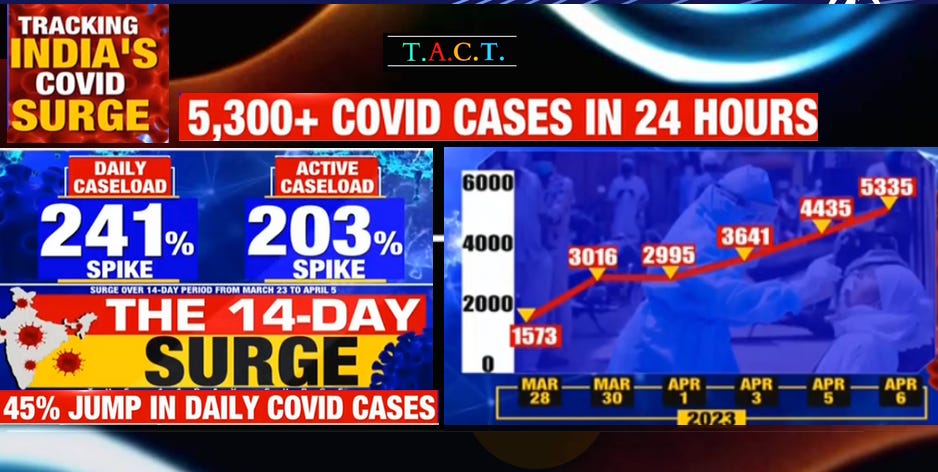
India reported 4,435 new cases on April 4th and 5,335 on April 5th, which is the highest in over 6 months. Exponential growth continues to gain momentum with a 241% spike in daily cases and a 203% spike in the active caseload over the past 14 days. The graph below illustrates how fast the latest variant is spreading. India is only testing a small fraction of people, so it's not the number of cases that is concerning, but the rate of growth.

Mask mandates are back in some states, but this time we're talking about Indian states. As they see a sharp increase in new cases, they are requiring everyone to wear masks in healthcare settings and at any event over 100 people. They are asking people to wear masks in any crowded situation in order to limit transmission. If exposed, wearing a quality N-95 or KN-95 mask tight around the nose and face will significantly reduce the viral load someone is exposed to, if not preventing an infection altogether. Remember that antibodies do not block these variants, so every particle inhaled must be eliminated by T cells after they infect a cell. We lose more cells the more viral particles that are inhaled. This alone causes COVID accelerated aging. The higher the viral load someone is exposed to, the greater the risk of persistent infections, and for younger children, it could mean long-term damage to the immune system.
This surge is occurring in a population heavily exposed to BA.5, XBB, and XBB.1.5. Those variants haven’t resulted in a significant surge in cases or deaths. That is what makes this more concerning. The number of cases is reportedly doubling every 4-5 days. This goes to show how much XBB.1.16 is able to evade prior immunity.
XBB.1.5 is able to evade antibodies. It defeated all of the available monoclonal antibody treatments. The question is, how can XBB.1.16 cause exponential growth when XBB.1.5 didn’t? The likely answer is that T-cells have effectively eliminated new infections in most people. However, based on the mutations that XBB.1.16 (.1) has acquired, this variant likely takes another bite into the T-cell response, our last layer of defense. The deaths, although still low in overall numbers, are also increasing at an exponential pace. Eleven more deaths were recorded on April 4, 2023, and thirteen on April 5, 2023. The states where XBB.1.16 was sequenced earliest, like Maharashtra, are seeing the most new cases and deaths.
On the other side of the world, in New Jersey, a state where XBB.1.16 was sequenced in late February, is reporting 618 new cases and 5 new deaths. There were 355 patients with confirmed or suspected cases reported across the state’s 70 hospitals on April 4th. Of those hospitalized, 47 are in intensive care and 20 are on ventilators. Long-term care facilities are reporting active outbreaks at 189 facilities, with 5,555 current cases among residents and 3,649 cases among staff, according to the latest data. We will watch NJ over the coming weeks to use as a measure of what to expect in the U.S. as prevalence builds.
On the Radar: XBB.1.31
XBB.1.31" is a variant that has been detected in a few locations worldwide, including Singapore, Indonesia, and the U.S. While it is still early to assess the level of threat it poses, there are reasons to be concerned. Alabama and California have reported cases of this variant as of March 13, 2023, but more sequencing is required to know the extent of its spread. Currently, an estimate of an 800% growth advantage is worrisome, even though it is based on only a few cases. That estimate will very likely be cut in half as more data becomes available. Even if cut in half, that is a huge advantage. The new mutations in XBB.1.31 suggest a higher growth rate and increased immune evasion capabilities by evading T-cells and antibody escape. XBB.1.31 carries mutations like K478R from XBB.1.16 and T547I from XBB.1.16.1, which has a 170% growth advantage. Additionally, it has the same ORF9b mutations, namely I5T, P10S, and N55S as XBB.1.16.
XBB.1.31 and S:Y453F Mutation
XBB.1.31 has acquired the Y453F mutation in the spike which isn’t in any of the XBB variants. The Y453F mutation was first found in the B.1.1.298 lineage, which was first sequenced in Denmark in April 2020. The lineage peaked in Denmark from October to November 2020 before declining, with the last sequence containing the Y453F mutation found in Denmark on January 18, 2021.
There is a study that found that COVID patients transmitted SARs-COV-2 to minks in the Netherlands in April 2020. Subsequently, the mink-associated virus (miSARS-CoV-2) spilled back over into humans. “Genetic sequences of the miSARS-CoV-2 identified a new genetic variant known as "Cluster 5" that contained mutations in the spike protein. The Y453F mutation located in the RBD domain of miSARS-CoV-2 is an adaptive mutation that enhances binding to mink ACE2 and other orthologs of Mustela species without compromising, and even enhancing, its ability to utilize human ACE2 as a receptor for entry. The Y453F spike exhibited resistance to convalescent serum, posing a risk for vaccine development.”
A study from 2020 found that virus variants with the Y453F mutation partially escaped detection by four neutralizing monoclonal antibodies and increased the binding affinity to ACE2 receptors. We still don’t know how this mutation will impact XBB.1.31 but based on what we know, it cause for concern.
S:Y453F Mutation Gained Independently in Immunocompromised
A study from 2021 revealed that a lymphoma patient with long-term COVID-19 exhibited an independent gain of 18 new mutations over more than 4 months of the disease, including the S:Y453F and Δ69-70HV mutations (known as "the ΔF combination"), previously associated with mink-related clusters. Although the patient's lineage was not related to the mink cluster, the presence of both mutations at a medium rate indicates intra-host polymorphism.
According to the study, "The observed excess of changes in the spike protein, and in particular in the RBD, is consistent with the effect of these mutations on hACE2 binding and/or antibody avoidance; in addition, the abundance of nonsynonymous changes at other proteins may suggest cytotoxic T-lymphocyte escape." These mutations may help the virus evade T-cells, and immunocompromised individuals are at greater risk for developing such mutations.
However, we have failed to adequately protect the immunocompromised, who have been protecting themselves and others. The trend we are seeing now is that new variants are adding or changing mutations to further evade our immune system. While the human body is capable of fighting infections, there is a limit. COVID-19 is evolving in a direction that is testing those limits, and we are in a state of inaction at a time when action is necessary. Given the mutations and growth rates, XBB.1.31 needs to be monitored closely.
It is crucial that we take immediate action to protect vulnerable populations and prevent the spread of COVID-19. This includes increasing funding for research and treatments that do not rely solely on mRNA, implementing stronger surveillance and screening measures, and prioritizing the installation of CO2 monitoring, ventilation, and filtration in high-risk settings. We must also take a proactive approach to detect and respond to new variants and localized outbreaks, rather than waiting until it is too late.
Attention Leaders at Every Level of Government
"Leaders at every level of government have a responsibility to anticipate and confront threats before they become catastrophic and engage the American people on the best course of action. Failure to do so could result in the loss of millions of lives and trillions of dollars." These words, spoken by President Bush in 2005, ring true today in the wake of the COVID-19 pandemic.
However, the current administration, led by President Biden, has failed to adequately address the ongoing crisis. Millions of Americans are being repeatedly infected with increasingly dangerous COVID-19 variants, causing immense harm and loss. Despite the warnings and rising numbers of cases in India and other countries, most leaders remain in a state of inaction, failing to fund treatments and vaccines that could prevent infection.
Although President Biden promised increased funding for Long COVID research and increased surveillance through testing and genomic sequencing, most proposed studies are not being funded, and the number of sequenced cases has declined. The CDC's guidance is incomplete, allowing new variants to enter the U.S. without proper screening and protection for vulnerable populations.
The Biden administration has not prioritized the installation of CO2 monitoring, ventilation, or filtration in schools, hospitals, or long-term care homes, nor have they implemented policies that provide an early warning of new variants or localized outbreaks. Despite talk of being on the right side of history, President Biden is failing to take the necessary actions to protect Americans, leaving future generations to bear the consequences of this inaction.
It is crucial that world leaders step up and take immediate action to protect their citizens. We cannot afford to wait any longer.
Independent sources that are not beholden to corporations, large donors, political parties, or any other group are more important than ever. Consider becoming a paid subscriber to help support this work.
T.A.C.T. is a publication supported by its readers. Consider becoming a free or paid subscriber if you are not already a member of the T.A.C.T. community.
Please share your thoughts and insights. Let us know how COVID is impacting you or anyone you know. What are you seeing in your area?
