



A False Promise? Review of Pfizer Booster for Children Under 5
The evaluation of the trial data leaves us with more questions than answers


This paper, published in The New England Journal of Medicine, February 16, 2023, evaluates the Pfizer booster’s safety and efficacy in children younger than 5 years of age. Before coming to the conclusion shown in the picture above, there are some important questions that need to be answered. Let’s dig into this.
“Evaluation of BNT162b2 Covid-19 Vaccine in Children Younger than 5 Years of Age”
Results: “The 3-μg dose level was selected for the phase 2–3 trial; 1178 children 6 months to less than 2 years of age and 1835 children 2 to 4 years of age received BNT162b2, and 598 and 915, respectively, received placebo.”
“Immunobridging success criteria for the geometric mean ratio and seroresponse at 1 month after dose 3 were met in both age groups.”
What is Immunobridging?

They are measuring antibody responses after one month, but we know that antibody levels decline rather quickly from one to three months. A concerning issue that they failed to mention is that the XBB variants are able to evade the antibodies that are induced by vaccines or previous infections. More on this below, but first, let’s look at what they wrote regarding the safety and efficacy.
Safety: “BNT162b2 reactogenicity events were mostly mild to moderate, with no grade 4 events. Low, similar incidences of fever were reported after receipt of BNT162b2 (7% among children 6 months to <2 years of age and 5% among those 2 to 4 years of age) and a placebo (6 to 7% among children 6 months to <2 years of age and 4 to 5% among those 2 to 4 years of age).
Efficacy: “The observed overall vaccine efficacy against symptomatic COVID-19 in children 6 months to 4 years of age was 73.2% (95% confidence interval, 43.8 to 87.6) from 7 days after dose 3 (on the basis of 34 cases).”
Their conclusion: “A three-dose primary series of 3-μg BNT162b2 was safe, immunogenic, and efficacious in children aged 6 months to 4 years.”
T.A.C.T.’s Review: Their conclusion sounds great; but we have some big issues to go over. They say that their conclusion is based on results from positive cases that occurred at least 7 days after dose 3 and before the data cutoff date.
They shared that the starting point was February 7, 2022, and the cutoff date was June 17, 2022. This is the time of year when cases declined in 2020 and 2021, so it is interesting that the efficacy trial was during this period. We can look at hospitalizations during this time and see they were already in steep decline by February 7, 2022. The decline happens every year at roughly the same time, so it is hard to believe that they didn’t time the trial for this period on purpose, but maybe it was just a coincidence.


Their conclusion is based on a trial that happened at a time of year when cases had declined the prior two years; whether by coincidence or not, this could affect the results. The trial conveniently concludes as cases start increasing again. The next issue is that their conclusion is based on older variants. They said the majority of the cases were caused by BA.2 and BA.2.12.1. They didn’t mention that COVID has evolved a lot since then and that XBB sub-variants evade antibodies from boosters and prior infections.
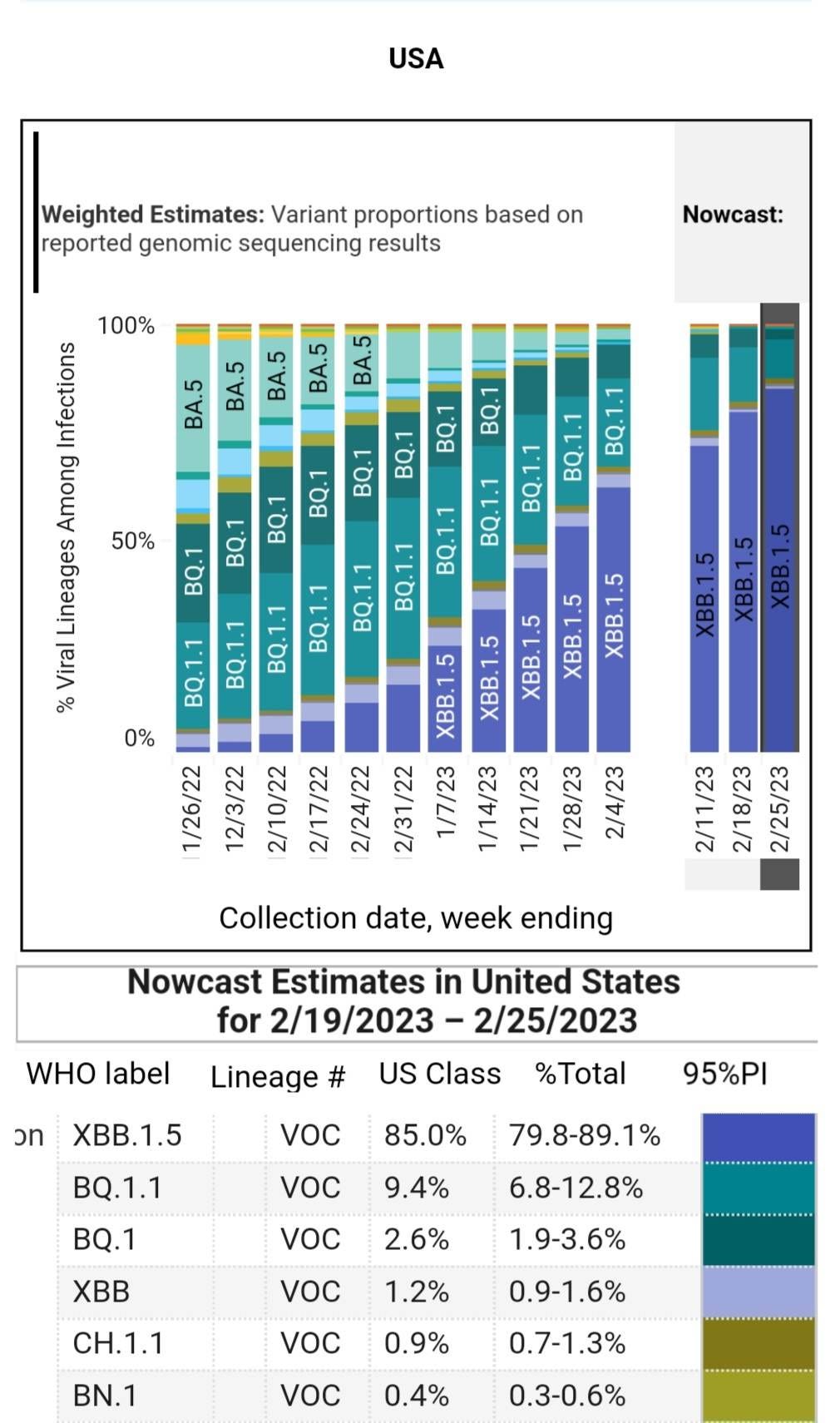
Just in case you are wondering, XBB.1.5’s prevalence is around 85% across the U.S., but some regions have up to 97% prevalence. There is a very good chance that this is the variant you have if you are infected with COVID. Canada hasn’t updated variant proportions since February 5th, but at that time XBB.1.5 looked like it was on course to be the dominant variant by now in most areas.
If antibodies don’t stop infections, then the virus can move into cells throughout the body before T-cells respond to kill the infected cells. That is a much more invasive process that won’t necessarily prevent persistent infections.
This trial evaluation looked at the antibody responses, but we know they aren’t adding much, if any, benefit. Even if it did, it would be for a few months. The next layer of our immune system’s defense that the vaccine has helped adults with, is developing a memory T-cell response. A study published in January 2023, reviewed below, shows that children aren’t developing a robust memory T-cell response, thus not building a strong immunity, but instead using more “naive” T-cells to fight each infection.
"Adults but not children develop robust memory T cell responses to SARS-CoV-2."
This may be helpful from the standpoint of the original antigenic sin, or immune imprinting. This may be a benefit of how humans evolved, but if true, it has costly implications when children continue to get reinfected with more immune evasive and suppressive COVID variants that are capable of infecting the heart, the brain, the tonsils, the adenoids, multiple types of immune system cells, and even the thymus.
Read more about how COVID may be causing irreversible damage to children’s immune systems.

Did this evaluation look at T-cell responses? No, it did not. That would have helped determine if there was any value in having young children take the vaccine.
T.A.C.T.’s Take: This data doesn't give enough information or take into account the other variables to support their conclusion. Lastly, the evaluation was “supported by BioNTech and Pfizer.” That presents a conflict of interest that adds greater suspicion to the points made here. This leaves us with more questions than answers, but at least we know what questions need to be answered in order to move forward.
Questions:
What are the memory T-cell responses at 1, 3, 6, 8, and 10 months? If they were not detected at 1 or 3 months, then those tests could obviously stop at that point.
What did the efficacy of this cohort look like at 6, 8, 10 months after the booster?
How many of the children were reinfected within 4, 6, 8, 10 months?
What are the antibody levels at 3, 4, or more months? It would be helpful to know this data, especially without T-cell data.
If any of this can be answered now, please share. Why aren’t they providing this data? We really need investment by these companies in finding a vaccine that prevents infections. They have made billions of dollars. Where are the next generation vaccines? What is their status? What are the government leaders doing about it, if anything? Those are some questions we'll dig into later, but please comment with questions, insight, and/or links if you have information.
Tracking the clonal dynamics of SARS-CoV-2-specific T cells in children and adults with mild/asymptomatic COVID-19
This study, published in January 2023, looked at mild and asymptomatic cases of COVID in children and adult family members and how this impacted the immune systems of children. All consented samples used in these analyses were collected between July 23 and October 24, 2020, so before the vaccines were used.
They found that "adults but not children develop robust memory T cell responses to SARS-CoV-2." Children do not have the same memory T-cell protection that adults develop, so that would leave them more exposed to reinfections, or it means they are using more naïve T-cells and damaging the development of the naïve T-cells that accumulate until puberty.
We continue down an unsustainable path for a large portion of the population. It is tragic to watch it unfold. It is like watching a tidal wave in slow motion, sweeping people up. Many people's feet are already off the ground as they are being pulled along, but they don't even know this is happening. Sadly, many will become disabled, many will die earlier than they otherwise would have, and others will tread water looking for solid ground. This is a preventable catastrophe. That’s what makes it all so much worse. Every week, hundreds of thousands of people become infected with the XBB.1.5 variant and other XBB sub-variants. An average of between 350 and 550 people are dying every day in the U.S. This is likely an undercount that doesn’t take into account the deaths from heart attacks, strokes, diabetes, cancers or dementia.
XBB.1.5 might appear milder to many people, but that doesn’t necessarily mean that people escaped injury or persistent infection. Check out the COVID Situation Simplified to get a better understanding of the situation.
